Prashanth Nandibewur1, Neeta Prashanth Nandibewur1
1Vijayanagara Institute of Medical Sciences (VIMS), Cantonment, Ballari, Karnataka 583104, (India)
Correspondence: Dr Neeta P N, Assistant Professor, C- 128, 5th Main, 3rd Cross, Opposite Vishnuvardhan Park, Kuvempnagar, Cantonment, Ballari- 583104 (India); Phone: 0-9844190501; E-mail: drnita10@gmail.com
ABSTRACT
Background: The fat embolism syndrome (FES) denotes clinical or subclinical respiratory insufficiency developing in patients with long bone fractures. It usually runs a mild course and responds well to measures for respiratory support. The subclinical form is detected by blood gas analysis and is associated with a PaO2 value of less than 60 mmHg. The present randomized double blind trial was conducted to evaluate the effectiveness of intravenous corticosteroids in comparison with placebo for the prevention of arterial hypoxemia in patients with long bone fractures.
Methodology: We conducted a double blinded randomized control trial among 44 patients, who showed signs and symptoms of sub clinical fat embolism and fulfilled our inclusion and exclusion criteria over 2 years period in a tertiary trauma care center. Forty four patients with long bone fractures were randomized as 21 in Group A (placebo group) and 23 in Group B (study group) respectively. The patients in the experimental group received a single dose of 30 mg/kg intravenous methylprednisolone upon admission to the emergency room. The control group received an equal volume of placebo (normal saline).
Results: The primary endpoints evaluated were the presence of fat embolism syndrome, based on the Lindeque’s criteria. Arterial blood gas (ABG) analysis showed PO2 of 67 ± 13 mmHg in Group A and 73 ± 8 mmHg in Group B. Mean arterial oxygen was not significantly different between the two groups (P = 0.09), this shows that single dose methylprednisolone (30 mg/kg intravenously) is effective as prophylaxis for prevention of arterial hypoxia in fat embolism syndrome. Among 44 patients studied 7 (33.33%) patients out of 21 in Group A manifested clinical FES. In Group B, 2 (8.7%) out of 23 patients had manifestations of the syndrome
Conclusion: Intravenous methylprednisolone administration to patients admitted with long bone fractures does not offer significant advantages in the maintenance of PaO2 and SpO2 levels when compared to placebo (normal saline), but reduces the frequency of development of fat embolism syndrome.
Key words: Arterial blood gas; Fracture, Methylprednisolone; Fat embolism syndrome
Citation: Prashanth N, Neeta PN. Effect of intravenous methylprednisolone in prevention of arterial hypoxemia due to fat embolism syndrome in patients with long bone fractures of lower limb – A double blind randomized trial. Anaesth Pain & Intensive Care 2016;20(3):290-294
Received: 12 May 2016; Reviewed: 18 May & 10 June 2016; Accepted: 15 September 2016
INTRODUCTION
Fat embolism syndrome (FES) is a respiratory deficiency syndrome due to decreased alveolar diffusion of oxygen. It occurs in three degrees of severity: a subclinical, an overt clinical, and a fulminating form. The subclinical fat embolism can be evaluated by peripheral oxygen saturation using pulse oximeter and arterial blood gases analysis.1
Arterial blood gas analysis showing an unexplained increase in pulmonary shunt fraction and an alveolar to arterial oxygen tension difference, especially within 24–48 h of a sentinel event associated with FES, is strongly suggestive of the diagnosis. Blood gases show hypoxia, with a PaO2 of less than 60 mmHg along with hypocapnia.2,3
Continuous pulse oximetry monitoring in high risk patients may help in detecting desaturation early, allowing early institution of oxygen and possibly steroid therapy; It would thus be possible to decrease the chances of hypoxic insult and systemic complications of FES.4 Preoperative use of methylprednisolone may prevent the occurrence of FES.5
Hypoxia is common after long bone fractures and may pass unnoticed.2,7 There is no clinical or experimental study until now to demonstrate beneficial effect of any drug on the clinical course of the syndrome,8 so that prevention, early diagnosis and adequate symptomatic treatment are the mainstays of treatment of this condition. Several pharmacological agents have been used as prophylactic treatment, such as hypertonic glucose,9 aspirin,5 dextrans5 and corticosteroids with variable results.1,9,10
Rokkanen was the pioneer in utilizing steroid prophylactically in an attempt to reduce the incidence of FES following massive trauma. This was followed by the interesting piece of evidence provided by Kreis et al. who demonstrated that corticosteroid improves oxygenation and decreases the pathologic changes seen on pulmonary biopsies in experimental animals. 11
The PaO2 reflects oxygen diffusion from the alveoli to the lung capillaries which is essential for tissue oxygenation. For this reason we used the PaO2 values to compare the effectiveness of methylprednisolone against a placebo. Owing to the subjective and variable nature of clinical diagnostic criteria, we mainly assessed objective findings suggestive of FES, including the presence of hypoxia. Accordingly, the present study evaluated the effectiveness of methylprednisolone in the prevention of development of FES, arterial hypoxia, in patients with long bone fracture(s).
METHODOLOGY
A randomized double blind placebo-controlled trial was performed on 44 patients with long bone fractures, who showed symptoms suggestive of subclinical FES, over a period of one year, May 2009 to May 2010, in a tertiary care hospital. The study included patients aged 16 to 46 years, presenting to our emergency room during the first 24 hours of the fracture. Patients were excluded if they had following systemic or chronic disease; pathologic fracture, pregnancy, previous steroid treatment, fractures with compartment syndrome, or they had accompanied head, chest, or abdominal trauma. Institutional ethical clearance was obtained and written informed consent was taken from all the study subjects.
The patients were randomized to experimental and control groups, the experimental group received a single intravenous dose of 30 mg/kg methylprednisolone over one hour in the emergency room, while the patients in the control group received placebo, consisting of 50 ml intravenous normal saline over one hour. Randomization was performed as follows: 50 envelopes were prepared, with 25 as Group A (placebo group) and 25 as Group B (study group). On admission, patients who fulfilled the inclusion and exclusion criteria, were assigned randomly one envelope and segregated to respective group by the third investigator (nursing staff) and administered the drug methylprednisolone or normal saline accordingly. As a result, we got only 44 patients, among these 21 in Group A (placebo group) and 23 in Group B (study group). The patients were followed up by the principal investigator in the ICU and in the wards. The group allocation was disclosed at the end of the study. Serial physical examinations and laboratory tests including arterial blood gas analyses were performed on admission and monitored sequentially (day 1 and day 2). All the patients underwent surgical fixation of bones i.e. intramedullary nailing within 12 hours. FES was diagnosed based on the Lindeque’s criteria.1
- A sustained PaO2 of less than 8 kPa (60 mmHg) with FiO2 0.21
- A sustained PaCO2 of more than 7.3 kPa (55 mmHg) or pH of less than 7.3
- A sustained respiratory rate of greater than 35 breath/min. even after adequate sedation
- Increased work of breathing as judged by dyspnea, use of accessory muscles, tachycardia and anxiety
Any patient with fracture femur and/or tibia showing one or more of these criteria was judged as having FES.
Data were analyzed and expressed in terms of rates, ratios and percentages. The statistical evaluation was accomplished using the unpaired t-test. A p < 0.05 was considered significant.
RESULTS
Forty four patients completed the study. Of these, 37 patients had fracture femur (84.1 %) while seven patients had fracture tibia (15.9 %).
In the experimental group, two patients developed FES (8.7%), whereas in the control group, seven patients developed the syndrome (33.33%). Mean age of Group A patients was 26.95 years and 28.78 years for Group B. Majority of patients (76.19% in Group A and 86.96% in Group B) were males.
On admission, the mean PO2 in Group B was 63.30 ± 4.55 mmHg (range: 53.0-71.0 mmHg) and 60.81 ± 4.93 mmHg (range: 51.0-70.0 mmHg) in control group. Statistical analysis revealed that there was no significant difference in the number of patients with arterial hypoxemia or mean arterial oxygen pressure, PCO2 and pH values (Table 1).
Table 1: Arterial blood gas analysis of patients in two groups on admission, day 1 and day 2
| Arterial Blood Gases | Group A | Group B | t Statistic | P value |
| Mean ± SD | Mean ± SD | |||
| PO2 on Admission | 60.81 ± 4.93 | 63.3 ± 4.54 | -1.73 | 0.9 |
| PO2 on Day 1 | 62.76 ± 5.71 | 64.87 ± 5.99 | -1.19 | 0.24 |
| PO2 on Day 2 | 66.81 ± 13.07 | 73.48 ± 8.51 | -1.98 | 0.05 |
| PCO2 on Admission | 34.57 ± 4.56 | 33.43 ± 5.63 | 0.73 | 0.46 |
| PCO2 on Day 1 | 35.62 ± 3.62 | 33.57 ± 3.97 | 1.79 | 0.08 |
| PCO2 on Day 2 | 35.9 ± 4.23 | 34.7 ± 2.6 | 1.12 | 0.27 |
| PH on Admission | 7.32 ± 0.05 | 7.33 ± 0.05 | -1.39 | 0.2 |
| PH on Day 1 | 7.33 ± 0.03 | 7.34 ± 0.03 | -1.48 | 0.15 |
| PH on Day 2 | 7.33 ± 0.04 | 7.35 ± 0.23 | -1.67 | 0.11 |
.
.
.
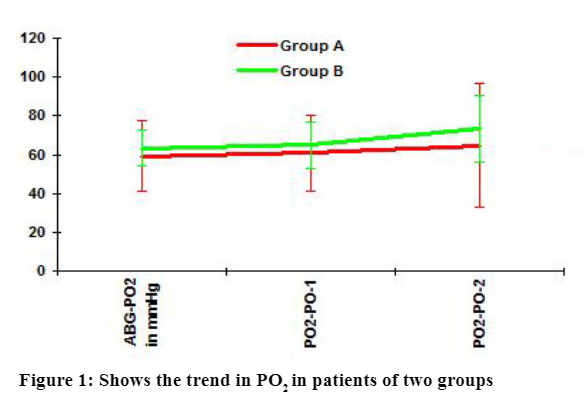
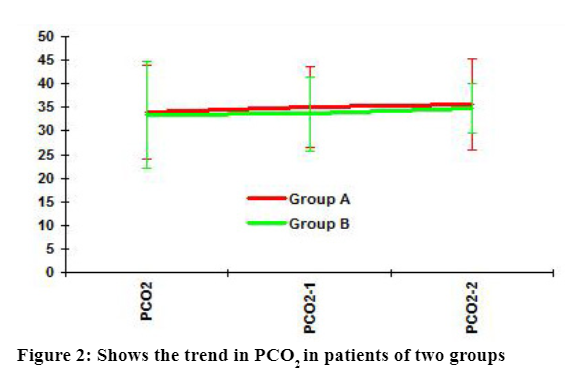
The arterial blood gas analysis showed a PO2 of 61 mmHg and 63 mmHg and PCO2 of 34 mmHg and 33 mmHg on admission in Group A and Group B respectively. Post operatively arterial blood gases (ABG) shows a PO2 of 67 ± 13 mmHg in Group A 73 ± 8 mmHg in Group B. PCO2 did not show a variation in two groups (Figure 1).
In the experimental group, all 23 patients had an initial baseline PaO2 value of more than 53 mmHg; in two of them, this fell to below 55 mmHg on day one and in two on day 2 during the trial. In the control group, 20 patients had baseline PO2 of more than 55 mmHg; in two of them, PO2 fell below 55 mmHg during day 1 and in seven patients below 55 mmHg on day 2. This difference was not statistically significant (Figure 1).
Arterial blood gas analysis on admission showed mean PO2 of 60.81 mmHg in Group A and 63.3 mmHg in Group B: the mean PCO2 levels were 34.57 mmHg and 33.43 mmHg; and the pH was 7.32 and 7.33 in the two groups respectively (Figure 2).
.
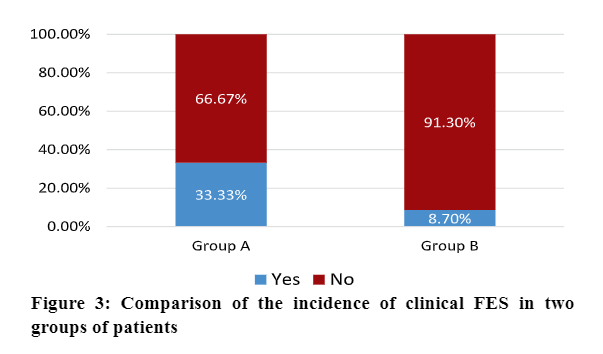
Among 44 patients studied 7 (33.33%) patients out of 21 in Group A manifested clinical FES. In Group B 2 (8.7%) out of 23 patients had manifestations of the syndrome (Figure 3).
DISCUSSION
Hypoxemia is one of the important signs of fat FES. Tachakra et al6 studied relation between hypoxia and fractures of femur and tibia. They studied fifty patients with fractures of lower limb and pelvis. Arterial blood gas analysis showed a phase of hypoxia in 32 out of 50 fracture patients without head, chest or abdominal injury. The PO2 in this hypoxemia was between 60 to 70 mmHg. He concluded that pulmonary fat embolism is the most likely explanation of the hypoxemic episodes.
The treatment of FES is difficult due to lack of specific diagnostic indicators. Symptomatic treatments such as protecting critical tissues and organs (such as the lungs and brain), correcting hypoxemia, respiratory support, and prevention of complications were performed as major therapeutic measures, death and disability remain major threats to these patients.12,13 Prevention is essential and improves the success rate of treatment and reduces the rate of disability.14,15
The arterial blood gas (ABG) values on room air in these patients showed mean values of PO2 61 mmHg, PCO2 33 mmHg and pH 7.32. The PO2 values were similar to that obtained by Tachakra et al.6 This overall picture of hypoxemia following long bone fracture was suggestive of fat embolism. Another study showed much higher PO2 levels.13
Collins14 reported that arterial PO2 fell below 80 mmHg in one third of 33 patients with comminuted femoral shaft fractures. Bradford et al15 found arterial oxygen saturation below 90% in eight out of 23 patients in one or more fractures of tibia and femur. McCarthy et al16 observed a fall in PaO2 below 80 mmHg during first two days after injury in 28 out of 50 patients with fractures of the extremities. In our study we found no significant difference between the two groups with regard to number of patients with arterial hypoxemia or mean arterial oxygen pressure.
One study stated that methylprednisolone succinate, in a single dose of 10 mg/kg, was not effective in prevention of FES, although it decreased its incidence. Corticosteroid therapy has been recommended in selected cases in patients with multiple or bilateral long bone fractures.13 We used a higher dose of 30 mg/kg of methylprednisolone prophylactically in anticipation of better effect than the lower dose used by earlier investigators. May be because of that our results were more favorable in preventing FES as well as maintaining arterial blood gas levels.
The incidence of clinical FES in study group patients (8.7%) was significantly lower (chi square test, p = 0.0430) than that in control group patients (33.3%). Our study demonstrated that methylprednisolone 30 mg/kg significantly reduces the incidence of FES when given as a single prophylactic dose. This is in close agreement to the study by Antti Alho and colleagues17 where methylprednisolone 30 mg/kg was given in divided doses.
CONCLUSION
In summary, use of methylprednisolone 30 mg/kg does not show statistically significant improvement in the arterial blood gas values, but the incidence of fat embolism syndrome is reduced in this group than in the placebo group. The routine early administration of intravenous methylprednisolone to patients admitted with long bone fractures offers advantages in the maintenance of PaO2 and SpO2 levels and a reduction in the incidence of the fat embolism syndrome.
Acknowledgements: We thank our hospital staff members and patients for participating in our study.
Conflicts of interest: None declared.
Authors’ contribution: Both authors took equal part in the concept, conduct of the study and the manuscript preparation.
REFERENCES
- Lindeque BG, Schoeman HS, Domisse GF, Boeyens MC, Vlok AL. Fat embolism and the fat embolism syndrome.A double blind therapeutic study. J Bone Joint Surg Br. 1987 Jan;69(1):128–31. [PubMed]
- Babalis GA, Yiannakopoulos CK, Karliaftis K, Antonogiannakis E. Prevention of posttraumatic hypoxaemia in isolated lower limb long bone fractures with a minimal prophylactic dose of corticosteroids. 2004 Mar;35(3):309-17. [PubMed]
- Sheikh N. Emergency management of fat embolism syndrome. J Emerg Trauma Shock. 2009 Jan;2(1):29–33. doi: 10.4103/0974-2700 [PubMed] [Free full text]
- Wong MV, Tsui HF, Young SH, Chan KM, Cheng JC. Continuous pulse oximeter monitoring for in apparent hypoxemia after long bone fractures. J Trauma. 2004 Feb;56(2):356–62. [PubMed]
- Schonfeld SA, Ploysongsang Y, DiLisio R, Crissman JD, Miller E, Hammerschmidt DE, et al. Fat embolism prophylaxis with corticosteroid: A prospective study in highrisk patients. Ann Intern Med. 1983 Oct;99(4):438–43. [PubMed]
- Tachakra SS, Sevitt S. Hypoxaemia after fractures. J Bone Joint Surg Br. 1975 May;57(2):197-203. [PubMed]
- Moed BR, Boyd DW, Andring RE. Clinically inapparent hypoxaemia after skeletal injury. The use of the pulse oximeter as a screening method. Clin Orthop Relat Res. 1993;(293):269—73. [PubMed]
- Richards RR. Fat embolism syndrome. Can J Surg. 1997 Oct;40(5):334—9. [PubMed] [Free full text]
- Shier M, Wilson RF, James RE, Riddle J, Mammen EF, Pedersen HE. Fat embolism prophylaxis: a study of four treatment modalities. J Trauma. 1977 Aug;18(8):621—9. [PubMed]
- Kallenbach J, Lewis M, Zaltzman M, Feldman C, Orford A, Zwi S. ‘Low-dose corticosteroids’ prophylaxis against fat embolism. J Trauma. 1987 Oct;27(10):1173-6. [PubMed]
- Sen RK,Tripathy SK, Krishnan V.. Role of corticosteroid as a prophylactic measure in fat embolism syndrome: a literature review. Musculoskelet Surg. 2012 Jun;96(1):1–8. doi: 10.1007/s12306-011-0156-1[PubMed]
- Mobarakeh MK, Saied AR, Scott RK. Efficacy of Corticosteroids in Prevention of Fat Embolism Syndrome in Patients with Long Bone Fracture. Iran J Med Sci. 2008;33(4):240-243. [Free full text]
- Collins JA. The causes of progressive pulmonary insufficiency in surgical patients. J Surg Res. 1969 Dec;9(12):685-704. [PubMed]
- Kubota T, Ebina T, Tonosaki M, Ishihara H, Matsuki A. Rapid improvement of respiratory symptoms associated with fat embolism by high-dose methylpredonisolone: a case report. J Anesth. 2003;17(3):186-9. [PubMed]
- Han YY, Sun WZ. An evidence-based review on the use of corticosteroids in peri-operative and critical care. Acta Anaesthesiol Sin. 2002 Jun;40(2):71-9. [PubMed]
- Robert JH, Hoffmeyer P, Broquet PE, Cerutti P, Vasey H. Fat embolism syndrome. Orthop Rev. 1993 May;22(5):567-71. [PubMed]
- Alho A,Saikku K, Eerola P, Koskinen M, Hämäläinen M. Corticosteroids in patients with a high risk of fat embolism syndrome. Surg Gynecol Obstet. 1978 Sep;147(3):358–62. [PubMed]