
Santiago M Herrero, MD, FCCP*, Joseph Varon, MD, FACP, FCCP, FCCM, FRSM**
*Gijón General Hospital (Hospital of Cabuenes), Principality of Asturian Health System (SESPA), University of Oviedo, Government Principality of Asturias, 33203 Gijón, Asturias (Spain)
**The University of Texas Health Science Center, Chief of Critical Care Services, University General Hospital, Clinical Professor of Medicine, The University of Texas Medical Branch at Galveston, Houston, TX 77030 (USA)
Correspondence: Santiago M Herrero MD, FCCP, Intensive Care Unit, Hospital Cabuenes, Calle Los Prados 395, 33203 Gijón, Asturias (Spain); Tel: +34 985185000 (Ext: 85144-85133); Fax: +34 984102696; E-mail: drsantiagoherrero@gmail.com; http://infouci.org
ABSTRACT
Therapeutic hypothermia (TH) has gained popularity in recent years for its use in a variety of clinical situations, and currently is one of the major fields of investigation. Mild TH is the process of decreasing the core body temperature between 32-34°C in those patients with acute brain injury, such as those who survive a cardiac arrest but remain comatosed. Different methods and devices are available to induce systemic TH, however, over the past decade, other possibilities including cooling the brain without reducing the core body temperature (selective brain hypothermia) have evolved in an attempt to minimize potential systemic adverse effects.
Keywords: Cardiac arrest; Neuroprotection; Therapeutic hypothermia; Selective brain hypotermia
Citation: Herrero SM, Varon J. Therapeutic hypothermia: lessons and obstacles in neuroprotection. Anaesth Pain & Intensive Care 2013;17(3):225-227
Each year in the European Union, approximately 275,000 to 375,000 people suffer from a cardiac arrest outside the hospital, with wide differences in survival, ranging from 0-30%.1 Marrugat and coworkers, estimated that in Spain there were nearly 9,000 sudden cardiac deaths in 1999 among the population aged 25 to 74 years.2 Approximately 12% of all natural deaths occur suddenly and 88% of them are of cardiac origin. In Spain, the numbers of sudden cardiac deaths are difficult to account, especially as the population has increased by 7 million people over the last 10 years. This figure would likely be higher if death certificates were accurate.3 In 2011, it was estimated that 25,500 to 36,000 people suffered sudden cardiac arrests (54-76 per 100,000 population), which was four times more than the deaths attributable to traffic accidents.4
When a literature search was conducted utilizing PubMed (National U.S. National Library of Medicine) with the descriptors “Therapeutic Hypothermia” And “After Cardiac Arrest”, 2325 publications were found since 1957, of which 1489 had been performed in humans, 842 in the last 5 years, 278 were full reviews, and 168 clinical trials. This indicates the relevance of TH and the reason why it is currently one of the major fields of basic and clinical research.
Goals of Therapeutic Hypothermia
The preservation of the brain function is the final goal of resuscitation after cardiac arrest. Unfortunately, most of these patients do not recover from the resultant anoxic brain insult. Several animal and human trials have suggested that TH improves neurologic recovery after cardiopulmonary arrest.
The historical development of TH dates back millennia; however, its use in modern clinical medicine has been documented for the last 200 years.5 TH was introduced in the 1950s as a protective measure for the brain, and has been used routinely in the operating room in an attempt to provide prolonged neuroanesthesia.6–8 Benson and collaborators, first described in 1959, the effective use of TH after cardiac arrest, after applying to 12 patients.9 Years later, Professor Peter Safar, in the early 1960’s, recommended TH as an important part of the assistance after resuscitation. However, it was not until 2002 when two randomized, controlled, clinical trials documented a significant improvement in survival without neurological damage with TH as compared with normothermia in patients with out of hospital cardiac arrest and coma.10-11
After these clinical trials, the International Liasion Committe on Resuscitation (ILCOR) recommended its use in those patients victims of cardiac arrest with return of spontaneous circulation (ROSC) that remained comatosed, in which ventricular fibrillation (VF) was the intial rhythm.12
Today, TH (whole body or selective head cooling), is recognized as standard of care for brain injury control in term infants with perinatal hypoxic ischemic encephalopathy (HIE).13
This therapeutic modality has gained ground in clinical medicine, especially when applied to other clinical conditions, in which patients may have an acute or diffuse brain damage.8,14 Among the potential indications: near drowning, traumatic cardiac injury, rhythms other than VF (asystole, complete heart block or pulseless ventricular tachycardia), stroke, central nervous system infections, hepatic encephalopathy, status epilepticus, heart failure and the adult respiratory distress syndrome have been suggested.
Additional experimental work is needed to determine whether TH is always beneficial in the treatment of septic shock and myocardial infarction.15
Surface Cooling Devices For TH
A variety of methods are available to accomplish TH. Surface cooling devices are non-invasive methods and range from simple ice applications, cooling blankets, ice packs to highly sophisticated machines with automatic feedback control. Newer devices have cooling rates comparable to invasive intravenous catheter techniques. Invasive cooling methods include the administration of ice-cold fluids intravenously, intravascular cooling catheters, body cavity lavage, extra-corporeal circuits and selective brain cooling.16
How Does TH Help?
For every degree drop in body temperature, the cerebral metabolic rate decreases by 6-7% . Likewise there is an improvement in oxygenation in those ischemic areas of the brain as well as, decreasing intracranial pressure and decreasing postreperfusion injury.17-18
The primary objective of the TH is to prevent further damage to prevent secondary brain dead after primary brain injury. After brain insult, the primary damage is inevitable and that injury will lead to a permanent lesion. We can prevent secondary lesions using TH as a neuroprotective treatment. Prevention of the secondary lesion (which affects the prognosis) and whose injury is undervalued, could affect cognitive impairment favorably (Figure 1).
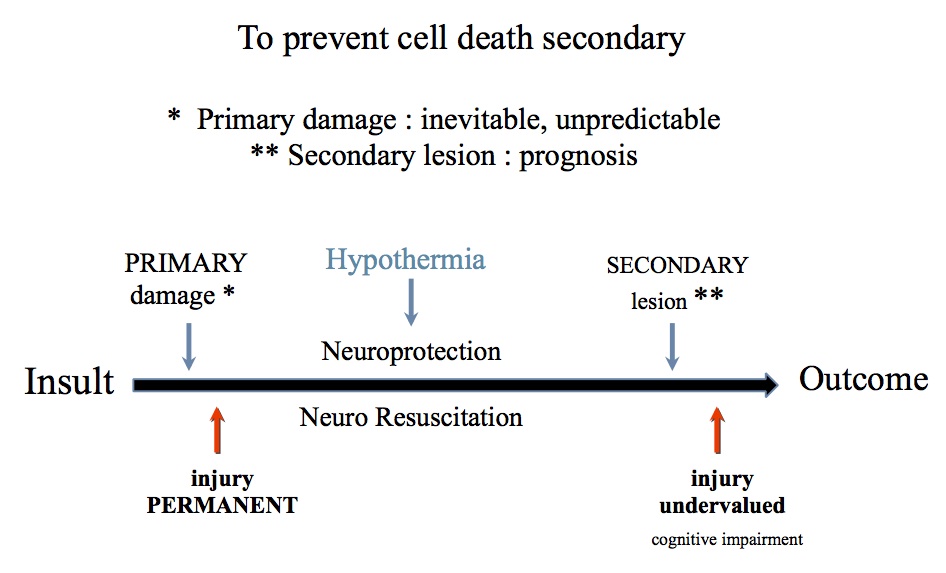
Figure 1:
TH reduces the free radicals (ROS), excitatory neurotransmitters, destructive enzymatic reactions, intracellular acidosis and maintains the integrity of the lipoproteic membrane.19
The importance of the temperature decrease, the rate at which it is accomplished and its precise neuroprotective role has not been fully and clearly evaluated; however, a rapid induction of TH will improve cognitive prognosis.
Controversies in TH
TH confers a small risk associated with a variety of undesirable side effects, regardless of the methods used. Several studies have reported complications with the use of therapeutic hypothermia particularly at lower temperatures (<32 ºC) and with an uncontrolled maintenance of temperature.20 Among these, dysrhythmias, infections and primary coagulopathy are the most commonly cited.12,21 The ‘Hypothermia After Cardiac Arrest’ (HACA) study group reported sepsis as the main complication with TH, however, this did not reach statistical significance.12
Some authors recommend avoiding TH in patients with severe cardiogenic shock or life-threatening dysrhythmias, pregnant patients or patients with a primary coagulopathy.16 In the authors’ personal experience, none of these are absolute contraindications and clinicians must use their clinical judgement as TH has been proven useful in all of these conditions.
Selective brain cooling (SBH) may be able to avoid many undesirable effects observed during systemic TH.
The Future of TH
To date, practically all studies on SBH have been performed experimentally in animals, and there are only 20 reports in humans using different methods of cerebral cooling.
Natale and associates, in 1989, performed SBH using nasal lavage with water at 5 °C in dogs with complete cerebral ischemia induced by 10 min of cardiac arrest and noted that this technique, significantly ameliorated neurologic morbidity and mortality.22
Anecdotal cases are reported in human adults, but there is greater experience in the use of SBH in the hypoxic-ischemic newborn. The usual noninvasive methods for inducing SBH range from neck pads with instant ice packs as a transitional method for TH to upper airway heat loss or heat loss through the skull using fans or caps, cool hats and helmets to invasive methods as antegrade cerebral perfusion, intracarotid flush, opening the brain surface and irrigating closed or semiclosed areas of the brain ventricles or direct contact of specific areas of the brain.23
Ice packs are can be used in ambulances and emergency departments, and can lower the brain temperature while only dropping core temperature by 1.5 to 2 °C.23
Other selective brain cooling methods are cool head and neck pads (heat sinks), with thermal conductivity of 70 W/mk (100 times more conductive than conventional cooling pads) and produce a rapid induction whose effects are notable within 2 min.
The latest methods for selective brain cooling is using a intranasal cooling system (Rhino Chill®), which delivers high pressure iced gas and cooled mixture to the patients through a sterile tubing set, of single use device. Poli and co-investigators, in a prospective, observational study using the Rhino Chill® device for nasopharyngeal cooling in stroke patients, observed that the device cooled the brain efficiently, however, steep increases in blood pressure raise serious concerns regarding the safety of its use.24
Another device system using balloon catheters are inserted into the nostrils and the circulation of a cold saline fluid system design in a closed loop, inducing the brain to be cooled rapidly, has been tested in healthy volunteers in a preliminary study (Varon J, Personal communication).
In conclusión, the best possible technique and the optimum use of therapeutic hypothermia, still need a lot of research for its full authentic use in prolonging human life.
REFERENCES
- Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-of-hospital cardiac arrest and survival rates: Systematic review of 67 prospective studies. Resuscitation. 2010;81:1479-87. [PubMed] doi: 10.1016/j.resuscitation.2010.08.006. Epub 2010 Sep 9.
- Marrugat J, Elosua R, Gil M. Epidemiología de la muerte súbita cardíaca en España. Rev Esp Cardiol. 1999;52(9):717-25. [PubMed] [Free full text]
- Varon J, Sternbach GL. Cardiopulmonary resuscitation: lessons from the past. J Emerg Med 1991;9,503-507. [PubMed]
- Sealy WC, Brown IW Jr, Young WG Jr. A report on the use of both extracorporeal circulation and hypothermia for openheart surgery. Ann Surg 1958;147:603–613. [PubMed] [Free full text]
- Kawamura S, Suzuki A, Hadeishi H, et al. Cerebral bloodflow and oxygen metabolism during mild hypothermia insubarachnoid haemorrhage. Acta Neurochir (Wien) 2000;142:1117-1121. [PubMed]
- Bernard SA, Buist M. Induced hypothermia in critical care medicine: A review. Crit Care Med 2003;31:2041-2051. [PubMed]
- Benson DW, Williams GR, Spencer FC, Yates AJ. The use of hypothermia after cardiac arrest. Anesth Analg. 1959;38:423-8. [PubMed]
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N Engl J Med. 2002;346:557-63. [PubMed] [Free full text]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med. 2002;346:549-56. [PubMed] [Free full text]
- Nolan JP, Morley PT, Vanden Hoek TL, Hickey RW, et al. Therapeutic hypothermia after cardiac arrest. An advisory statement by the Advanced Life Support Task Force of the International Liaison Committee on Resuscitation. Circulation 2003;108:118-21. [PubMed] [Free full text]
- Gancia P, Pomero G. J. Brain cooling and eligible newborns: should we extend the indications? Matern Fetal Neonatal Med. 2011;24 Suppl 1:53-5.
- Mayer SA, Sessler DI: Therapeutic hypothermia. Marcel Dekker Ed. New York, NY 2005.
- Safar PJ, Kochanek PM. Therapeutic hypothermic after cardiac arrest. N Engl J Med 2002;346:612-3. [PubMed] [Free full text]
- Holzer M. Devices for rapid induction of hypothermia. Eur J Anaesthesiol 2008;42:31-8. [PubMed] doi: 10.1017/S0265021507003274.
- Rosomoff HL, Holaday DA: Cerebral blood flow and cerebral oxygen consumption during hypothermia. Am J Physiol 1954;179:85-88. [PubMed]
- Kawamura S, Suzuki A, Hadeishi H, Yasui N, Hatazawa J. Cerebral blood flow and oxygen metabolism during mild hypothermia in patients with subarachnoid haemorrhage. Acta Neurochir. 2000;142:1117-21. [PubMed]
- Salazar-Reyes H, Varon J: Hypoxic tissue damage and the protective effects of therapeutic hypothermia. Crit Care & Shock 2005;8:28-31.
- Alzaga A, Cerdan M, Varon J. Therapeutic hypothermia. Resuscitation 2006;70:369-380. [PubMed]
- Hypothermia after Cardiac Arrest Study Group. The hypothermia after cardiac arrest study group: mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N Engl J Med 2002;346:549-56. [PubMed] [Free full text]
- Natale JA, D’Alecy LG. Protection from cerebral ischemia by brain cooling without reduced lactate accumulation in dogs. Stroke. 1989;20(6):770-7. [PubMed] [Free full text]
- Harris BA, Andrews PJD. Direct brain cooling. In: Mayer S, Sessler DI (Eds): Therapeutic Hypothermia. New York, Marcel Decker. 2005:323-386.
- Poli S, Purrucker J, Priglinger M, Sykora M, Diedler J, Rupp A, et al. Safety Evaluation of Nasopharyngeal Cooling (RhinoChill®) in Stroke Patients: An Observational Study. Neurocrit Care. 2013 Sep 12. [PubMed]
- Curós Abadal A. Parada cardíaca extrahospitalaria, nuestra asignatura pendiente. Rev Esp Cardiol. 2001;54:827-30. [PubMed] [Free full text]
- Inēbase Database. National Statical Institute of Spain. Available from URL: http://www.ine.es/jaxi/tabla.do. Accesed November 27, 2013.
