
Khalid Maudood Siddiqui1*, Ali Asghar1 and Kashif Munshi1
1Department of Anesthesiology, Aga Khan University Hospital, Stadium Road P. O. Box 3500, Karachi 74800, Pakistan
Correspondence: Dr. Khalid Maudood Siddiqui, Department of Anesthesiology, Aga Khan University Hospital, Stadium Road P. O. Box 3500, Karachi 74800, (Pakistan); E-mail: khalid.siddiqui@aku.edu
ABSTRACT
Primary cardiac tumors are an infrequent occurrence during infancy and childhood and the most common amongst the primary cardiac neoplasms are myxomas, which have an estimated incidence of approximately 2-3 per 100,000 population. The atrial myxoma has a preponderance to occur in the left atrium with only a 25% incidence in the right atrium. Depending upon the site and the size of the neoplasm, the clinical picture varies and may range from no significant symptoms to cardiac arrest. Hence, the diagnosis and management of this condition requires highly specialized multidisciplinary input by the perioperative caregivers including cardiologists, cardiothoracic surgeons, anesthesiologists and the nurses specialized to deal with this unique population. There is a dearth of available literature on the anesthetic management of these primary intra-cardiac tumors with reports of neonatal right atrial myxoma excision a true rarity. We report the successful anesthetic management of one such case of a right atrial mass in an 18 days old female child.
Key words: Atrial mass resection; Atrial myxoma; Neonate; Diagnosis; Cardiac surgery; Outcome
Citation: Siddiqui KM, Asghar A, Munshi K. Early diagnosis and resection of right atrial mass in a neonate. Anaesth Pain & Intensive Care. 2016;20 Suppl 1: S161-S164
Received: 25 August 2016; Reviewed: 1 September 2016; Accepted: 10 September 2016
INTRODUCTION
Primary cardiac tumors are uncommon in infancy and childhood. Autopsy studies in children reported an incidence of 0.03% to 0.08%.1 Even the most common primary tumour, cardiac myxoma is estimated to occur in fewer than 2 to 3 people per 100,000 population.2 There is little information available related to anesthetic management of neonate with primary cardiac tumors. The case is presented, since no such case of myxoma resection in neonate has been reported yet in literature.
CASE REPORT
We are presenting a case of 18 days old female neonate weighing 3.2 Kg, who was born in local hospital with normal vaginal delivery. According to the mother her pregnancy was uneventful. She was her third child and other two siblings were normal. This baby was born with APGAR score of 8 and 9 after 1 and 5 minutes respectively. After birth her general and physical examination was unremarkable except that the pediatrician was alerted by the frequent missed heart beats on auscultation. A Trans thoracic echocardiography was planned which exhibited a huge mass seen in right atrium measuring 18x8mm adjacent to the opening of superior vena cava with no obstruction to flow. It further showed multiple small masses in both ventricles close to the interventricular septum measuring 4×2 mm and 3×2 mm each side, with normal left ventricle systolic function and patent foramen ovale.
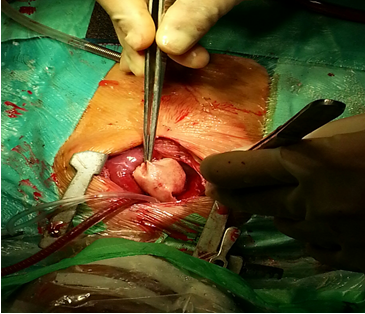
Figure 1: Bovine graft during atrial reconstruction.
Later, the child was shifted to tertiary care hospital for further management. On her monitoring ECG showed atrial arrhythmias; it was relieved spontaneously without any intervention. At 16th day of her birth the MRI was done which showed right atrial mass measuring up to 17x23mm; attached to the free wall of right atrium without causing any obstruction along with normal anatomy of great vessels with normal left and right ventricles functions. On the basis of Transthoracic echocardiography and MRI the provisional diagnosis of myxoma or rhabdomyoma was made and surgical resection was planned under general anesthesia.
On preoperative evaluation the baby had stable vital signs, was afebrile and active, her weight was 3.5 kg. Her complete blood count and electrolytes were in normal range. The routine monitoring of ECG, NIBP, SpO2 and end tidal CO2 (Datex Ohmeda AS, Helsinki, Finland) were applied and induced with Sevoflurane 8% along with 100% Oxygen. Injection fentanyl 10 µg and atracurium 1.5 mg were given intravenously through already placed 24G cannula in her right hand. After complete muscle relaxation, we intubate the child with PVC tube size 3 mm ETT on direct laryngoscopy by McIntosh blade size 0. Her Intubation grade was I on Cormack and Lehane classification. Bilateral air entry was confirmed with auscultation. Anesthesia was maintained with oxygen and air 50% each and isoflurane 1.5% MAC along with fentanyl infusion 5 µg/kg/hr on controlled mode of ventilation. After induction the arterial line was put with 22 G (Vygon, UK) cannula on her right femoral artery and central venous pressure line 4F, 5 cm (Arrow, USA) in right femoral vein taken with all aseptic measures.
After handing over the patient to the surgeon, median sternotomy was performed, patient was heparinized with 1200 IU and aorto-bicaval bypass was established. Patient was put into cardiopulmonary bypass. The aorta was cross clamped and antegrade root cardioplegia was given. The heart stopped in diastole. Then right atriotomy was performed, the mass was excised completely (Figure 1) and remaining defect in right atrial wall was reconstructed with bovine pericardial patch. We specifically advised to perfusionist to achieve dilutional ultrafiltration (DUF) and zero-balance ultrafiltration (Z-BUF); it is effective for the removal of inflammatory mediators and also reduces the pulmonary and myocardial dysfunction. The child was gradually weaned off from cardiopulmonary bypass. Protamine 10 mg was infused to neutralize the heparin. Her hemodynamic parameters were stable throughout the surgery; the epinephrine infusion 0.05 µg/kg/min was also started to support the stunned myocardium. During surgery patient’s serial ABGs were normal in range without any evidence of acidosis. At the end of surgery patient went into supraventricular tachycardia. Adenosine 200 µg/kg was given through central line. She responded well and supraventricular tachycardia was terminated. Her hemoglobin and electrolytes was kept within a normal range. Patient was then shifted to cardiac intensive care unit (CICU) and weaned off after few hours. She was discharged from CICU to special care unit after 48 hours.
DISCUSSION
Around 75% of primary cardiac tumors are benign. Although atrial myxomas are rare but these are the most common benign tumors of the heart, ranging upto 50%. Lipomatous hypertrophy of interatrial septum, lipomas, papillary fibroelastoma of tricuspid valve and hemangiomas can also arise from any heart chamber.3 All these tumors usually arise more from the left atrium. A myxoma usually appear as a sessile or pedunculated tumor with a smooth and friable surface. Areas of hemorrhage are also visible in few cases. They have rarely been defined as originating in early stage of life.4
Primary heart tumors and pericardium are more significant for their native effects than for their potential metastatic behavior. The complications endorsed to such tumors depend on their location, size, movement, flexibility, friability, and the invasiveness of tumor progression. Myxoma may result compression of heart structures, valvular insufficiency, outflow tract obstruction, coronary emboli and occasionally sudden cardiac death.5
Due to the low incidence and the variety in clinical presentation, the diagnosis of primary cardiac tumors may be overlooked or delayed, this explains the morbidity and mortality associated with benign cardiac tumors. Right atrial myxoma has been previously reported in a neonate, which showed symptoms similar to cyanotic heart disease and the baby expired without having any diagnosis. Autopsy finding revealed large atrial mass causing complete obstruction in tricuspid valve area.6 Myxoma might cause unspecific general symptoms such as arthralgias, fever, fatigue and anemia, because of released tumor yields such as interleukin-6, tumor necrosis factor or other neuroendocrine factors from the neoplastic tissue. Clinical examinations are otherwise non-specific, however cardiac signs in patients who have no previous cardiac issues in association with general symptoms and embolic events should initiate cardiac investigation. Echocardiography always considered as first on investigations list.7 Magnetic resonance imaging (MRI) generally permits a complete tumor diagnosis and helpful to the planning of operative procedure and surgical resection is indicated in every patient.8 Whole hospital mortality after resection of atrial myxomas should be less than 2-3%. Almost, all mortalities are found in older age patients with severe comorbidities. Supraventricular arrhythmias (SVT) are relatively frequent after resection of atrial tumors. Recurrence is very rare and may be caused by an inadequate excision or growth from a new foci.9
Arrhythmias due to conduction defects are common in patients with atrial myxomas. It has been postulated that the mechanical expansion of the atrium and the relative hypoxia caused by the tumor compression may result in conduction defects and other arrhythmias. Additionally the anesthesiologist should be cautious of the fact that there could be difficulty in the insertion of the central venous line in the atrium due to the presence of the tumor, and complications like hypotension, arrhythmias and embolization are more expected during central line insertion. Another important cause of hypotension in these patients is outflow obstruction due to changing with position. As the myxoma is mobile within the atrium, certain positions may cause complete obstruction of the AV outflow tract.10 To certain extent this can be evaluated preoperatively as patients are more symptomatic in those positions. However, a very carefully monitored positioning and titrated induction technique should always be employed, and all preparations to go into an emergent cardiopulmonary bypass if required should be done even before anesthetic induction to avoid disastrous situations. Tumor embolization should be avoided as emboli of right-sided myxomas can obstruct pulmonary arteries, cause acute pulmonary hypertension and even cause death from acute obstruction. Precautions should be taken during SVC cannula insertion and during the placement of central venous line to avoid entering into the right atrium due to the risk of tumor fragmentation and embolization.11 Transesophageal echocardiography (TEE) is recommended intraoperatively to aid in recognizing and avoiding embolization. All intravenous tubing should be free of air to avoid paradoxical embolization.9
CONCLUSION
Intra-cardiac myxomas account for a small percentage of cardiothoracic surgeries and the paucity of such surgeries accounts for the limited experience with the patient population presenting with such conditions. Early diagnosis with careful perioperative planning and a multidisciplinary approach towards the management of such patients even when encountered in the neonatal age can translate into successful patient outcome with a lower morbidity and mortality.
Conflict of interest: None
Authors’ Contribution: KMS – Conduction of study work, manuscript writing; AA – Perioperative anesthesia care, literature search and manuscript editing; KM – Perioperative anesthesia care and literature search
REFERENCES
- Kussman BD, Devavaram P, Hansen DD, DiNardo JA, Forbess JM, Mehrota R, et al. Anesthetic implications of primary cardiac tumors in infants and children. J Cardiothorac Vasc Anesth. 2002;16(5):582-6. [PubMed] doi:10.1053/jcan.2002.126952
- Carrel T, Erdös G, Eberle B, Englberger L, Pfammatter J-P, Schmidli J, et al. Surgical treatment of cardiac tumors-an overview and presentation of interesting cases. Cardiovascular Medicine. 2011;14:242-57. [Free Full Text]
- Kaul P, George R, Paniagua R, Balaji S, Sivananthan M, Sapsford R. Massive inferior venacavo-atrial thrombus following neoadjuvant chemotherapy. Br J Cardiol. 2012;19(4):184. [Free Full Text] doi:10.5837/bjc.2012.034
- Maruf M, Akter T, Islam F, Chowdhury A, Khan J, Hassan K, et al. Left Atrial Myxoma in a Child: An Uncommon Presentation of a Rare Tumour in Early Age. Cardiovasc j. 2011;4(1):99-101. [Free Full Text]
- Nomura K, Nakamura Y, Uno Y, Yamashiro M. Pediatric Left Atrial Myxoma: Surgical Excision and Mitral Valve Plasty. Ann Thorac Cardiovasc Surg. 2007;13(1):65. [PubMed] [Free Full Text]
- Dianzumba SB, Char G. Large calcified right atrial myxoma in a newborn. Rare cause of neonatal death. Br Heart J. 1982;48(2):177. [PubMed] [Free Full Text]
- Reeder GS, Khanderia BK, Seward JB, Tajik AJ. Transesophageal echocardiography and cardiac masses. Mayo Clinic Proceedings. 1991;66(11):1101-9. [PubMed] doi:10.1016/S0025-6196(12)65788-7
- Shah DJ. Evaluation of cardiac masses: the role of cardiovascular magnetic resonance. Methodist Debakey Cardiovasc J. 2010;6(3):4-11. [PubMed] doi: 10.14797/mdcj-6-3-4
- Murayama H, Tamaki S, Kato N, Yuji N, Yokote J, Mutsuga M, et al. Right atrial myxoma associated with atrial septal defect: a case report and review of the literature. Ann Thorac Cardiovasc Surg. 2001;7(3):166-9. [PubMed]
- Balachander RSH, Badhe A, Chandran B: Anesthetic Management of a patient with right atrial myxoma – A Case Report And Anesthetic Considerations. The Int J Anesthesiol.2009: 26(1). [Free Full Text]
- Battellini R, Bossert T, Areta M, Navia D. Successful surgical treatment of a right atrial myxoma complicated by pulmonary embolism. Interact CardioVasc Thorac Surg. 2003;2(4):555-7. [PubMed] [Free Full Text] doi: 10.1016/S1569-9293(03)00133-6
