
Rajeev Chauhan, MD1, Suman Arora, MD2, Surender K. Malhotra, MD2, Kiran Jangra, MD3, Ashok K. Gupta, MS2
1Senior resident; 2Professor; 3Assistant Professor
Department of Anesthesia & Intensive care, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh (India)
Correspondence: Dr Kiran Jangra, Assistant Professor, Department of Anesthesia & Intensive Care, Post Graduate Institute of Medical Education & Research (PGIMER),
Chandigarh-160012 (India); Phone: +91-9914844330; Fax: 0091-172-2744401; E-mail: drkiransharma0117@gmail.com
ABSTRACT
Objectives: Hypotensive anesthesia is necessary during endoscopic sinus surgery to achieve a bloodless surgical field. The aim of this study was to compare the quality of surgical field using propofol or desflurane anesthesia.
Methodology: 40 patients of either sex, belonging to ASA physical status I and II and age group of 18 – 60 years were randomized into two groups to receive either propofol and morphine or desflurane and morphine anesthesia. The target mean arterial pressure (MAP) was kept in a range of 65-75 mmHg. The quality of surgical field was assessed by using a validated scoring system (Fromme category scale) at every 15 min by the same surgeon in all the cases to avoid surgeon’s bias.
Results: The mean category scale value was 2.665 ± 0.243 in propofol group and 2.200 ± 0.410 in desflurane group (p=0.000). The time to emergence was significantly less in desflurane group (9.35 ± 1.27 min) as compared to propofol group (14.60 ± 2.06 min).
Conclusion: We conclude that both the propofol and desflurane can be used to achieve a satisfactory surgical field quality but desflurane provides a rapid emergence as compared to propofol.
Key words: Controlled hypotension; Endoscopic sinus surgeries; Desflurane; Propofol
Citation: Chauhan R, Arora S, Malhotra SK, Jangra K, Gupta AK. Comparison of surgical field quality and emergence time during endoscopic sinus surgery using propofol or desflurane: A randomized clinical trial. Anaesth Pain & Intensive Care 2016;20(3):285-289
Presented in the International Anesthesia Research Society (IARS) conference held on May 4-7, 2013 at San Diego (USA).
INTRODUCTION
Chronic sinus diseases are common public health problem that affects the quality of life of more than 5% population1. Approximately 12.5% of the population in US experience this disease at least once during their lifetime2. Chronic sinusitis accounts for substantial loss of work days and health care expenditure. An important anesthetic consideration during endoscopic sinus surgery (ESS) is to provide blood less field as, even a small amount of bleeding can hamper the visibility of operating surgeon and increases the risk of complications like intraorbital hemorrhage, injury to optic nerve, ocular muscle, intracranial hemorrhage and dura, cerebrospinal fluid leak, and meningitis.3-6 The anesthesiologists are encouraged to provide controlled hypotension or low normal blood pressure with the mean arterial pressures (MAP) between 65-75 mmHg. As controlled hypotension provides a relatively blood less surgical field, facilitates surgical dissection, decrease in bleeding with concomitant reduction in transfusions and decreases operative time.3,5,7
Various maneuvers and techniques are used to improve the quality of surgical field including reverse Trendelenburg position, decongestion of nasal mucosa, use of hypotensive agents and high spinal and epidural blocks.8 In previous studies various hypotensive agents has been used to produce controlled hypotension such as vasodilators such as sodium nitroprusside,9-11 nicardipine,9 nitroglycerine (NTG),9 β1-adrenergic blockers e.g. esmolol and metoprolol10,11 and high doses of inhalational agents such as isoflurane. All these techniques were associated with various side effects such as tachycardia, tachyphylaxis, cyanide poisoning, uncontrolled hypotension and rebound hypertension. So, anesthesiologists are still searching for the drugs that can provide better quality of surgical field with minimal side effects.
Various anesthetic agents influence the quality of surgical field and blood loss during surgery due to their hypotensive and vasodilatory action. There is an ample literature suggesting the superiority of propofol over inhalational agents (isoflurane, sevoflurane and desflurane) in ESS.12 The aim of present trial was to compare the use of propofol and desflurane for the surgical field conditions and emergence time in endoscopic sinus surgery.
METHODOLOGY
This prospective, randomized, single blinded trial was commenced after getting the institutional ethics committee approval and written informed consent from every patient or next of kin. This study was conducted from January 2011 to March 2012 at our institute. Forty patients with American Society of Anesthesiologists (ASA) physical status I or II, undergoing elective ESS for chronic sinusitis of varied origin, were enrolled in the study. Patients with a known history of major organ dysfunction (hepatic, renal or cardiovascular system), patients already on beta blockers or cardioactive drugs, pregnancy, recurrent sinus surgeries, bleeding disorders, and anticoagulation therapy were excluded from the study. Patients were randomized as per computer generated sample randomization code in two parallel groups [Group P (n = 20), Group D (n = 20)]. The sample size calculation was based on previous studies13 and included 20 patients per group to achieve a beta power of 80% and an alpha error of 0.05. The primary outcome included the comparison of quality of surgical field using either propofol or desflurane. The secondary outcomes included hemodynamic variability and time of emergence. Sealed envelopes were used to ensure allocation concealment. The surgeon assessing quality of surgical field was blinded to the agents used intraoperatively and the group assigned. After reaching in the operating room, intravenous (IV) line was secured and intraoperative monitors were attached including, pulse oximetry, direct arterial blood pressure, electrocardiogram, end tidal carbon dioxide, neuromuscular blockade and end tidal desflurane agent. After pre-oxygenation, patients were induced using morphine (0.1 mg/kg) and propofol (1-2.5 mg/kg) IV. Orotracheal intubation was facilitated by vecuronium (0.1 mg/kg) and oropharynx was packed with a saline-soaked throat pack. In Group-P (Propofol Group), anesthesia was maintained with propofol infusion 100-200 μg/kg/min and nitrous oxide (50%) in oxygen. While in Group-D (Desflurane Group), anesthesia was maintained with combined minimal alveolar concentration (MAC) value of 1-1.3 of desflurane (3-4%) and nitrous oxide (50%) in oxygen. The dose of maintenance agent was adjusted to achieve the target mean arterial pressure (MAP) of 65-75 mmHg. Rescue hypotensive agents, such as esmolol 5-10 mg and/or metoprolol 1-2 mg boluses or infusion of NTG (0.25–1.0 µg/kg/min), were used if target MAP was not achieved despite maximum allowable anesthetic agent concentration. The choice of rescue agent was based on the baseline vital characteristics of the patients; beta blockers were used for those who had tachycardia, while NTG was preferred for those whose baseline heart rate was lower, or in a few patients the combination of both was used. The patients requiring rescue agents were recorded in both the groups. Patients were monitored for persistent hypotension (MAP < 65 mmHg), bradycardia (heart rate < 45 beats/minute), postoperative nausea, vomiting and shivering. In those patients who developed hypotension, rescue drugs were stopped and fluids were infused rapidly and the dose of anesthetic agents was reduced. In the cases of severe hypotension or those who did not respond to above said maneuvers injection mephentermine was used in 3 mg increment bolus. Quality of surgical field was defined in relation with the bleeding in the surgical field and the need of suction to clear blood to get visibility under endoscope. The quality of operative field was assessed by using the A scale proposed by Fromme et al14 (Table 1). The category scale values of 2 and 3 in Fromme score were considered as ideal. The same surgeon assessed the quality of surgical field at every 15 min during the surgery in all the patients to remove subjective bias in the assessment.
Table 1: Surgical grade scoring system designed specifically for use in endoscopic sinus surgery
| Grade | Parameter / observation |
| Grade 0 | No bleeding. |
| Grade 1 | Slight bleeding – No suctioning required. |
| Grade 2 | Slight bleeding – Occasional suctioning required. |
| Grade 3 | Slight bleeding – Frequent suctioning required. |
| Grade 4 | Moderate bleeding – Frequent suctioning required. Bleeding threatens the surgical field immediately after suction is removed. |
| Grade 5 | Severe bleeding – Constant suctioning required. Bleeding appears faster than that can be removed by suction. Surgery is impossible. |
The data were analyzed by using the SPSS software for windows, version 13.0. Descriptive data were expressed as frequencies, median and mean with standard deviations. The variations in the heart rate and MAP within each group were analyzed and compared by using repeated measures ANOVA and Student’s t test. A p-value <0.05 was taken as statistically significant.
RESULTS
A total of 48 patients were assessed for eligibility to participate in the study. Of these 2 patients refused to participate in the study and 6 patients did not meet the eligibility criteria. A total of 40 patients were enrolled in the study. Demographic data was comparable with respect to sex, weight and ASA status except age. The mean age was 30.2 years in desflurane group and 44.3 years in propofol group (Table 2).
Table 2: Demographic data
| Parameters | Group 1
(Mean ± SD) |
Group 2
(Mean ± SD) |
p-value |
| Age (years) | 44.30 ± 17.38 | 30.20 ± 12.09 | .005* |
| Weight (Kg) | 65.15 ± 10.49 | 61.65 ± 14.423 | .386 |
| Sex (M/F) | 13/7 | 11/9 | .519 |
| ASA status (I/II) | 17/3 | 17/3 | 1.000 |
| Rescue drugs
(NTG/Metoprolol) |
9/20 | 4/20 | 0.091 |
* Statistically Significant (p<0.01), ASA-American Society of Anesthesiologists, NTG-Nitroglycerine.
The Values are expressed as mean ± SD and number of patients.
Table 3: Quality of surgical field and emergence time
| Parameter | Group P
(Mean ± SD) |
Group D
(Mean ± SD) |
p-value |
| Fromme scale | 2.665 ± 0.243 | 2.200 ± 0.410 | 0.000* |
| Emergence time (min) | 14.60 ± 2.06 | 9.35 ± 1.27 | 0.000* |
| Duration of
surgery (min) |
46.40 ± 11.93 | 45.70 ± 8.45 | 0.832 |
| Duration of
anesthesia (min) |
74.55 ± 12.20 | 69.85 ±10.19 | 0.194 |
* Statistically Significant (p<0.05), Group P- Propofol group, Group D-Desflurane group
The quality of surgical field was significantly better in Group-D as compared to Group-P (Table 3). The number of patients requiring rescue antihypertensive drugs to achieve target MAP (65-75 mmHg) was comparable between the two groups (Table 2). Target blood pressure was rapidly achieved and well sustained throughout the surgery in both the groups (Figure 1).
Figure 1: Comparison of mean arterial pressure between the groups
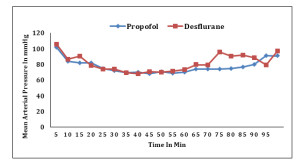
Heart rate was also comparable in both the groups. The mean duration of anesthesia and surgery were comparable between the two groups, but the time for emergence was significantly shorter in Group-D as compared to Group-P (Table 3). There was no incidence of refractory hypotension, bradycardia or any other complication in both of the groups.
DISCUSSION
Excessive bleeding that occurs due to the rich vascularity of the nose makes the surgical procedure difficult and lengthy and also increases the risk of serious complications such as orbital perforation or dural puncture.15 Hypotensive anesthesia during ESS helps to decrease these complications.16 In our study target blood pressure (65-75 mmHg) was achieved in both the propofol and desflurane groups and provided a satisfactory surgical field but emergence was more rapid in desflurane group than the propofol group.
The previous study by Chan et al17 demonstrated the improvement of the surgical field quality in SNP induced hypotension following a moderate reduction in MAP. Lim et al18 demonstrated that MAP lower than 70 mmHg leads to increased intraoperative bleeding due to local vasodilatation. Profound hypotension with MAP of 50 mmHg was avoided as Leigh et al19 have reported 0.02-0.06% mortality due to hypotension induced ischemic organ damage. In contrast, Boezaart et al20 found that profound hypotension (MAP = 50 mmHg) provided good surgical field during ESS. In our study we aimed the target MAP of 65-75 mmHg and achieved a significant improvement in surgical field quality.
Propofol was chosen as it had been demonstrated to decrease bleeding and provides a better quality of surgical field than the inhalational agents in patients undergoing ESS.13 Propofol depresses the cerebral blood flow and cerebral metabolic rate and maintains flow metabolism coupling.13 This reduction of cerebral blood flow might decrease blood flow to the paranasal sinuses closer to brain (ethmoid and sphenoid) and diminishes the bleeding related to arterial inflow. Propofol decreases the central sympathetic tone and causes vasodilation in peripheral blood vessels.21 Bonhomme et al22 showed that propofol may preferentially minimize the arteriolar bleeding and might not affect the venous bleeding significantly.
The inhalational agents decrease the systemic vascular resistance in dose-dependent manner leading to increased capillary bleeding despite the lower systolic blood pressure. Beaussier et al23 found that desflurane along with fentanyl provides better hemodynamic stability than isoflurane during moderate hypotensive anesthesia in spine surgeries. Desflurane is currently being used for hypotensive anesthesia.24 It causes decrease in arterial pressure as a result of reduction in left ventricular after load. Cardiac output is either not changed or slightly depressed with desflurane at 1-2 MAC. Hypotension induced compensatory tachycardia serves to maintain cardiac output despite modest decrease in stroke volume and contractility.
Both the propofol and desflurane decrease the MAP, stroke volume and systemic vascular resistance.25,26 Heart rate does not change significantly after injection of propofol, whereas rapid increase in desflurane concentrations exceeding 1 MAC might result in sympathetic stimulation and tachycardia. Due to the favorable recovery characteristics it was particularly interesting to investigate propofol or desflurane during controlled hypotension. The lower solubility of desflurane (blood gas partition coefficient of 0.42) results in the faster emergence after anesthesia.27
A meta-analysis by Gupta et al28 on emergence after either propofol or desflurane found only minor differences in reaching recovery goals or emergence. On contrary, in our study desflurane showed significant difference in emergence time probably due to higher dose requirement of propofol for obtaining desired MAP. Rohm et al29 also found faster recovery time and time to extubation with desflurane/fentanyl anesthesia as compared to propofol in open abdominal prostatectomy.
LIMITATIONS
There are a few limitations in our study. We did not classify our patients as per the invasiveness of the preoperative lesion. More extensive lesions (Lund Mackay > 12) have been shown to be associated with an increased blood loss and poorer surgical score.30 Also, the amount of blood loss is difficult to assess in ESS and we did not calculate it in our study.
CONCLUSION
Controlled hypotension and a satisfactory surgical field can be achieved with both desflurane and propofol but the emergence time is more rapid with the use of desflurane.
Conflict of interest: None declared by the authors
Authors’ contribution:
RC, SA, KJ, SKM & AKG: Concept, conduct of study work, preparation of manuscript
SA, SKM & AKG: Review of manuscript. KJ: Data collection
REFERENCES
- Pleis JR, Lucas JW, Ward BW. Summary health statistics for US adults: National Health Interview Survey, 2008. Vital Health Stat 10. 2009 Dec;(242):1–157. [PubMed] [Free full text]
- Infectious rhinosinusitis in adults: classification, etiology and management. International Rhinosinusitis Advisory Board. Ear Nose Throat J. 1997;76(12 Suppl.):1–22. [PubMed]
- Maniglia AJ. Fatal and other major complications of endoscopic sinus surgery. Laryngoscope. 1999 Apr;101(4 Pt 1):349-54. [PubMed]
- Stankiewicz JA. Complications of endoscopic intranasal ethmoidectomy. Laryngoscope. 1987 Nov;97(11):1270-73. [PubMed]
- Kennedy DW. Prognostic factors, outcomes and staging in ethmoid sinus surgery. Laryngoscope. 1992 Dec;102(12 Pt 2 Suppl 57):1-18. [PubMed]
- Lund VJ, MacKay IS. Outcome assessment of endoscopic sinus surgery. J R Soc Med. 1994 Feb;87(2):70-2. [PubMed] [Free full text]
- Gittleman PD, Jacobs JB. Skorina J. Comparison of functional endoscopic sinus surgery under local and general anaesthesia. Ann Otol Rhinol Laryngol. 1993 Apr;102(4 Pt 1):289-93. [PubMed]
- John G, Low JM, Tan PE, van Hasselt CA. Plasma catecholamine levels during functional endoscopic sinus surgery. Clin Otolaryngol Allied Sci. 1995 Jun;20(3):213-5. [PubMed]
- Degoute CS, Dubreuil C, Ray MJ, Guitton J,Manchon M, Banssillon V, et al. Effects of posture, hypotension and locally applied vasoconstrictor on the middle ear microcirculation in anesthetized humans. Eur J Appl Physiol Occup Physiol. 1994;64(5):414-20. [PubMed]
- Degoute CS, Ray MJ, Manchon M, Dubreuil C,Banssillon V. Remifentanil and controlled hypotension:Comparison with nitroprusside or esmolol during tympanoplasty. Can J Anaesth. 2001 Jan;48(1):20-7. [PubMed]
- Boezaart AP, van der Merwe J, Coetzee AR. Comparison of sodium nitroprusside- and esmolol-induced controlled hypotension for functional endoscopic sinus surgery. Can J Anaesth. 1995 May;42(5 Pt 1):373-6. [PubMed]
- Pavlin JD, Colley PS, Weymuller EA Jr, Van Norman G, Gunn HC, Koerschgen ME. Propofol versus isoflurane for endoscopic sinus surgery. Am J Otolaryngol 1999;20:96-101. [PubMed]
- Sivaci R, Yilmaz MD, Balci C, Erincler T, Unlu H. Comparison of propofol and sevoflurane anaesthesia by means of blood loss during endoscopic sinus surgery. Saudi Med J. 2004 Dec;25(12):1995-8. [PubMed]
- Fromme GA, MacKenzie RA, Gould Ab Jr, Lund BA, Offord KP. Controlled hypotension for orthognatic surgery. Anesth Analg. 1986 Jun;65(6):683-6. [PubMed]
- Shi GG,Li XG, Wang ZD. Severe complications in the treatment of chronic rhinosinusitis and nasal polyps with endoscopic sinus surgery. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi. 2007 Jan;42(1):19-22. [PubMed]
- Al-Mujaini A, Wali U, Alkhabori M. Functional endoscopic sinus surgery: Indications and complications in the ophthalmic field. Oman Med J. 2009 Apr;24(2):70-80 doi: 10.5001/omj.2009.18. [PubMed] [Free full text]
- Chan W, Smith DE, Ware WH. Effects of hypotensive anaesthesia in anterior maxillary osteotomy. J Oral Surg. 1980 Jul;38(7):504-8. [PubMed]
- Lim YJ ,Kim CS, Bahk JH, Ham BM, Do SH. Clinical trial of esmolol-induced hypotension with or without acute normovolemic hemodilution in spinal surgery. Acta Anaesthesiol Scand. 2003 Jan;47(1):74-8. [PubMed]
- Leigh JM. The history of controlled hypotension. Br J Anaesth. 1975 Jul;47(7):745-9. [PubMed] [Free full text]
- Boezaart AP, Van der MJ, Coetzee AR. Comparison of sodium nitroprusside- and esmolol induced controlled hypotension for functional endoscopic sinus surgery. Can J Anaesth. 1995 May;42(5 Pt 1):373-6. [PubMed]
- Kaisti KKL, Metsahonkala L, Teras M, Oikonen V, Aalto S, Jaaskelainen S. Effects of surgical levels of propofol and sevoflurane anaesthesia on cerebral blood flow in healthy subjects studied with positron emission tomography. Anaesthesiology. 2002 Jun;96(6):1358-70. [PubMed] [Free full text]
- Bonhomme V, Fiset P, Meuret P, Backman S, Plourde G, Paus T, et al. Propofol anaesthesia and cerebral blood flow changes elicited by vibrotactile stimulation. A positron emission tomography study. J Neurophysiol. 2001 Mar;85(3):1299-1308. [PubMed] [Free full text]
- Beassuier M, Paugam C, Deriaz H,Mestari M, Chandon M, Sautet A, et al. Haemodynamic stability during moderate hypotensive anaesthesia for spinal surgery, a comparison between desflurane and isoflurane. Acta Anaesthesiol Scand. 2000 Oct;44(9):1154-9. [PubMed]
- Kaygusuz K, Yildirim A, Kol IO, Gursoy S, Mimaroglu C. Hypotensive anaesthesia with remifentanil combined with desflurane or isoflurane in tympanoplasty or endoscopic sinus surgery: a randomised control trial. J Laryngol Otol. 2008 Jul;122(7):691-695. doi: 10.1017/S0022215107001545. [PubMed]
- Young CJ, Apfelbaum JL. Inhalational anaesthetics: desflurane and sevoflurane. J Clin Anaesth. 1995 Nov;7(7):564-77. [PubMed]
- Skues MA, Prys-Roberts C. The pharmacology of propofol. J Clin Anaesth 1989;1(5):387-400. [PubMed]
- Agoliati A, Dexter F, Lok J, Masursky D, Sarwar MF, Stuart SB. Meta-analysis of average and variability of time to extubation comparing isoflurane with desflurane or isoflurane with sevoflurane. Anesth Analg. 2010 May 1;110(5):1433–9. doi: 10.1213/ANE.0b013e3181d58052. [PubMed]
- Gupta A, Stierer T, Zuckerman R, Sakima N, Parker SD, Fleisher LA. Comparison of recovery profile after ambulatory anaesthesia with propofol, isoflurane, sevoflurane and desflurane: a systematic review. Anesth Analg. 2004 Mar;98(3):632–41 [PubMed]
- Rohm KD, Piper SN, Suttner S, Schuler S, Boldt J. Early recovery, cognitive function and costs of a desflurane inhalational vs. a total intravenous anaesthesia regimen in long-term surgery. Acta Anaesthesiol Scand. 2006 Jan;50(1):14-8. [PubMed]
- Ahn HJ, Chung SK, Dhong HJ, Kim HY, Ahn JH, Lee SM, et al. Comparison of surgical conditions during propofol or sevoflurane anaesthesia for endoscopic sinus surgery. Br J Anaesth. 2008 Jan;100(1):50-4. [PubMed] [Free full text]
