
Indira Kumari, MD1, Udita Naithani, MD2, Harsha, MD3, Yogendra Singhal, MD4, Khemraj Meena, MD2, Madhan Mohan. C, MBBS5
1Sr. Professor and Head; 2Associate Professor; 3Ex PG student; 4Assistant Professor; 5Junior Registrar
Department of Anesthesiology, Rabindra Nath Tagore (RNT) Medical College, Near Collectorate, Hospital Rd, Court Chouraha, Madhuban, Udaipur, Rajasthan 313001, (India)
Correspondence: Dr. Indira Kumari, MD, 101, Jai Lakshmi Apartments, New Bhopalpura, Udaipur, Rajasthan, (India); Phone: 9414176760; E-mail: dr_ikumari@hotmail.com
ABSTRACT
Objective: Alpha-2 adrenoceptorshave recently been used perioperatively for their sedative, analgesic, sympatholytic and cardiovascular stabilizing effects. The efficacy of clonidine as an adjuvant in providing monitored anesthesia care (MAC) for ear, nose and throat (ENT) surgeries has not been much investigated, so we conducted this study.
Methodology: In this prospective double blind randomized placebo controlled study, 90 patients posted for elective ENT surgeries under local anesthesia with MAC were included and divided into 3 groups of 30 each. In Group CBI patients received clonidine 3 µg/kg intravenous bolus followed by clonidine infusion at 0.3 µg/kg/hr. Patients of Group CB received clonidine 3 µg/kg bolus followed by placebo infusion and in Group P patients received placebo bolus followed by placebo infusion. All three Groups received similar premedication of intravenous midazolam 0.03mg/kg and fentanyl 2µg/kg. Demographic data, intraoperative vital parameters, observer’s assessment and alertness scale (OAAS) score for sedation, bleeding score, patient and surgeon satisfaction score, postoperative Aldrete score, visual analogue scale (VAS) score for analgesia, rescue sedative and analgesic consumption and complications were noted.
Results: OAAS score(0-noresponse to 5-awake), 10 min after infusion of study drug was significantly lower in Groups CBI (2.06 ± 0.61) and CB(2.83 ± 0.70) signifying superior sedation as compared to placebo Group (4.80 ± 0.40), (p=0.000). Intraoperative rescue sedative and analgesic consumption were significantly lower in GroupsCBI and CB, as compared to placebo group (p = 0.000). Mean heart rate (HR) and mean arterial pressure (MAP) were significantly lower in Groups CBI and CB as compared to Group P (p = 0.000). Intraoperative bleeding score(0-Nolbleeding to 4-modearte bleeding) was significantly lower in Group CBI (0.86 ± 0.68) and CB (1.36 ± 0.76) as compared to placebo (3.10 ± 0.54), p = 0.000. Surgeons and patients were more satisfied in clonidine Groups CBI and CB, (p = 0.000). Patients of Group CBI demonstrated better sedation profile, less bleeding score and higher satisfaction scores as compared to Group CB (p<0.05).
Conclusion: Being a safe, well tolerated, cheap and effective regime, our study favors the use of clonidine 3 µg/kg IV bolus followed by infusion of 0.3µg/kg/hr as an adjunct to conventional MAC regime of midazolam and fentanyl in ENT surgeries as it provides effective sedation and bloodless surgical field.
Keywords: Clonidine;Imidazole: Imidazolines; Adrenergic alpha-2 Receptor Agonists; Intraoperative Monitoring; Monitoring, Physiological; Patient Monitoring; Otolaryngology; Pain Measurement; Analogue Pain Scale; Assessment, Pain; Visual Analog Pain Scale
Citation: Kumari I, Naithani U, Harsha, Singhal Y, Meena K, Mohan CM. Clonidine as an adjuvant in monitored anesthesia care for ENT surgeries: A prospective, randomized, double blind placebo controlled study.Anaesth Pain & intensive Care 2015;19(3):260-268
INTRODUCTION
Monitored anesthesia care (MAC) typically involves administration of local anesthesia in combination with IV sedatives, anxiolytic and/or analgesic drugs.1 Today it is the first choice in 10-30% of all the surgical procedures.2 MAC is being applied for various ear, nose, throat (ENT) surgeries in which an adequate sedation and analgesia without respiratory depression are desired for comfort of both the patient and the surgeon.3 It is important to have a surgical field that is free of blood as far as possible to improve visibility and so as to reduce the incidence of complications.4 Local anesthetic techniques have many advantages like, early recovery, less postoperative pain, and of great importance is the surgeon’s ability to test hearing while in surgery.5
Several drugs have been used for MAC such as, midazolam, propofol and fentanyl.6 The most commonly reported adverse effects of midazolam are variability of patient response and respiratory complications.7 Combining midazolam with fentanyl or other opioids increases the risk of hypoxemia and apnea and addition of propofol may further exacerbate respiratory depression.8
Recently alpha-2 adrenoceptor agonists i.e. clonidine and dexmedetomidine have been used as an alternative to other IV sedatives. Dexmedetomidine is becoming more popular as MAC anesthetic,6 but justification of its use may be difficult as it is more costly.9 Clonidine, comparatively cheaper agent also produces dose dependent sedation, analgesia, anxiolysis without relevant respiratory depression, provides hemodynamic stability and decreases sympathetic outflow resulting in significantly reduced bleeding during ENT surgeries.10,11 The efficacy of clonidine in MAC is sparsely studied.12The present study was designed to evaluate the role of clonidine as an adjuvant in MAC for ENT surgeries.
METHODOLOGY
After approval of the institutional ethical committee, this prospective, randomized double blind placebo controlled study was conducted at M. B. hospital attached to RNT Medical College, Udaipur (India). Informed consent was taken from each patient.
All consecutive adult cooperative patients of ASA physical status I-II, of both sexes, between 18 to 60 years of age, scheduled for elective ENT surgery under local anesthesia during period of one year (Jan 2014 to Dec 2014) were included in the study and were the basis of sample size. Exclusion criteria were patients having uncontrolled hypertension, cardiovascular/ hepatic/ renal/ endocrine diseases, coagulation disorder or taking drugs for systemic illness, any allergy to the study drug, on anticoagulation treatment, morbid obesity etc.
Ninety patients who fulfilled the above inclusion criteria were the study population.They were divided into 3 groups of 30 each using serial number technique. In Group CBI patients received clonidine 3 µg/kg bolus followed by clonidine infusion at 0.3 µg/kg/hr. Patients of Group CB received clonidine 3 µg/kg bolus followed by placebo infusion and in Group P patients received placebo bolus followed by placebo infusion.
Patients were instructed to keep fasting for 6-8 hours. All the resuscitation and monitoring equipment and emergency drugs were keptready for management of any adverse reactions. On the morning of surgery, standard monitorse.g. ECG, noninvasive BP, and pulse oximetry, were applied to the patient and baseline values were recorded. Two peripheral IV cannulas were inserted at different sites on the same arm (opposite to the side of surgery), one for infusion of clonidine or placebo and the other for administration of fluid and other drugs. Ringer lactate 500 ml was infused before premedication.
All the three groups received similar conventional sedation regime of IV midazolam 0.03mg/ kg and fentanyl 2µg/kg, which was followed by bolus study drug administration over 10 min as per group allocation. Immediately after this, the infusion of study drug was started and the surgeon administered local anesthesia using lidocaine 2% with 1:200000 adrenaline. After 10 min of start of infusion patients were assessed for level of sedation using Observers Assessment of Alertness Sedation scale13 (OAAS, 0-5); a score ≤4 was considered acceptable to allow the start of surgery and any patients having score >4, received IV propofol 0.5 mg/kg bolus as rescue sedative and was repeated until OAAS score was ≤4 to allow the surgery to start. Infusion of the study drug was continued throughout the surgery and stopped 10 min before anticipated conclusion of surgery. Intraoperatively, propofol 0.5 mg/kg IV bolus was used as rescue sedative (if OAAS >4) and fentanyl 25 µg IV bolus was used as rescue analgesic(on complaint of pain). Heart rate (HR), mean arterial pressure (MAP), respiratory rate (RR), oxygen saturation (SpO2) were recorded immediately after bolus, 10 min after infusion and then every 15 min till completion of surgery.
After surgery patients were shifted to recovery room. Aldrete score14(0-10) was assessed in recovery room every 5 min, till score of 10 was achieved, which was the criteria to shift the patient to ward. Postoperative pain in post anesthesia recovery room was noted on visual analogue scale (VAS, 0-10), and VAS score of >3 was treated with tramadol 100mg IV. Episodes of vomiting were noted and treated with ondansetron 4mg IV.
Intraoperative bleeding was assessed by the surgeon using bleeding score15 (0-4) at conclusion of surgery; acceptable bleeding score being 0-2. Patients were asked to rate their experience with the sedation (or analgesia) they have received during surgery using a 7-point Likert verbal rating scale. This assessment of patient’s satisfaction with sedation and analgesia was performed just before shifting to ward to minimize the effects of sedation on patients judgment. Surgeons were also asked to rate their satisfaction with operative conditions and patient sedation, using the same scale at the end of surgery, acceptable satisfaction score of both the patient and surgeon being.5-7
Intraoperatively, hypotension (SBP <90 mmHg) was treated with fluid bolus and inj. mephentermine 6mg bolus, bradycardia (HR <60/ min) was treated with atropine 0.4 mg IV boluses, hypoxia (SpO2<92% on air) was treated with supplemental oxygen by venturi mask. If these effects persisted, clonidine infusion was stopped. Various scores used in the study are shown in Appendix 1.
The primary efficacy end point was the percentage of patients not requiring propofol for rescue sedation based on achieving and/or maintaining an OAAS score ≤4. Secondary end points were total amount of rescue propofol and rescue fentanyl, hemodynamic stability, bleeding score, overall patient and surgeon satisfaction and recovery and readiness for discharge. Continuous variables were presented as mean ± SD and compared using student’s t test and ANOVA, whereas categorical data were presented as number (proportion) and compared using chi square test. Data were analyzed using SPSS version16.0, with P<0.05 considered as statistically significant.
RESULTS
All the three groups were comparable regarding mean age, mean weight, sex, ASA grade, diagnosis,
|
Variables |
Group CBI |
Group CB |
Group P |
P value |
||
|
CBI/ CB |
CB/P |
P/ CBI |
||||
| Age (yr) |
34.03 ± 13.61 |
30.03 ± 10.20 |
31.33 ± 11.02 |
0.220 |
0.634 |
0.420 |
| Weight (kg) |
52.23 ± 8.15 |
53.80 ± 6.54 |
54.33 ± 6.38 |
0.437 |
0.773 |
0.205 |
| Sex(male/female)(n) |
11/19 |
16/14 |
16/14 |
0.991 |
0.993 |
0.999 |
| ASA (I/II) (n) |
25/5 |
27/3 |
26/4 |
0.999 |
0.999 |
0.999 |
|
Type of surgery n (%) |
||||||
| Tympanoplasty |
21 (70%) |
16(53.33%) |
15 (50%) |
|||
| Septoplasty |
3 (10%) |
8 (26.67%) |
8 (26.67%) |
|||
| Myringoplasty |
4 (13.33%) |
5 (16.67%) |
7 (23.33%) |
|||
| Tympanotomy |
2 (6.67%) |
0 (0%) |
0 (0%) |
|||
| Polypectomy |
0 (0%) |
1 (3.33%) |
0 (0%) |
|||
| Duration of susurgery(min) |
109.17 ± 22.82 |
103.67 ± 27.72 |
103.00 ± 26.44 |
0.309 |
0.925 |
0.357 |
type of surgery, duration of surgery and baseline vital parameters(P>0.05) (Table 1).
Table 1: Demographic characteristics in three groups
| Tympanoplasty |
21 (70%) |
16(53.33%) |
15 (50%) |
|||
| Septoplasty |
3 (10%) |
8 (26.67%) |
8 (26.67%) |
|||
| Myringoplasty |
4 (13.33%) |
5 (16.67%) |
7 (23.33%) |
|||
| Tympanotomy |
2 (6.67%) |
0 (0%) |
0 (0%) |
|||
| Polypectomy |
0 (0%) |
1 (3.33%) |
0 (0%) |
|||
| Duration of susurgery(min) |
109.17 ± 22.82 |
103.67 ± 27.72 |
103.00 ± 26.44 |
0.309 |
0.925 |
0.357 |
Data are presented as Mean ± SD or number (proportion)
Mean OAAS score10 min after study drug was significantly lower in Group CBI (2.06 ± 0.61) and CB (2.83 ± 0.70) as compared to Group P (4.80 ± 0.40), (p=0.000). Difference between Group CBI and CB was also significant (p=0.010) (Table 2). In Group P, 27 (90%) patients required intraoperative rescue sedation (propofol 0.5 mg/kg) to keep them sedated (OAAS≤4), with number of doses ranging from 1 – 4 times, leading to a total of 63 rescue sedative doses. Whereas in Group CB 6 (20%) and in Group CBI only 1 (3.33%) patientrequired a single dose of rescue sedative. Intraoperative rescue analgesic (fentanyl 25 µg) was required by 26 (86.67%) patients in Group P, with number of doses ranging from 1–4 times, leading to total of 62 rescue analgesic doses. Whereas in Group CB 6 patients (20%) and in Group CBI only 1 patient (3.33%) required a single dose of rescue analgesic. Intraoperative rescue sedative and analgesic requirement was significantly higher in placebo group as compared to clonidine Groups, p=0.000. However, it was comparable in both clonidine groups(Table 3).
Incidence of postoperative pain (VAS >3) in PACU was significantly higher in Group P (n = 23, 76.67%) as compared to Group C B (n = 4, 13.33%) and Group C BI (n = 0) (p = 0.000), who were given IV tramadol.Mean postoperative VAS score in PACU was in the order ofGroup P (4.46 ± 1.35) >Group CB (2.20 ± 1.31)≈Group CBI (1.70 ± 1.29).
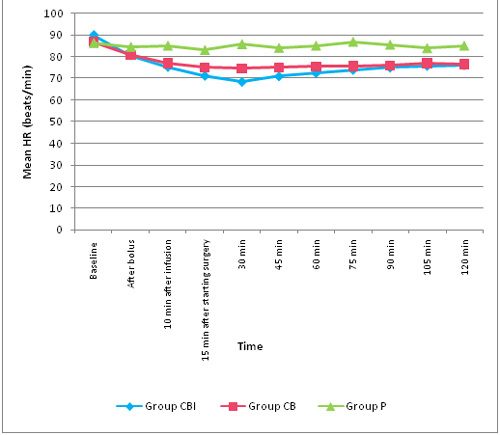
Mean heart rate showed significant fall from baseline at all time intervals in Groups C BI and C B (p<0.05) with maximum fall at 30min after starting surgery and it was 23.91% in Group C BI and 14.09% in Group CB. There was no significant variation from baseline in Group P with respect to heart rate (p>0.05).On inter-group comparison, mean heart rate was significantly lower in Group C BI and C B as compared to Group P throughout the surgery. Mean heart rate was significantly lower in Group C BI as compared to GroupCB from 15 min to 75 min of surgery (p<0.05). However, bradycardia (HR <60/min) was seen in only one patient (3.33%) of Group C BI. (Figure 1).
Fig 1: Comparison of mean heart rate (HR) during intraoperative period
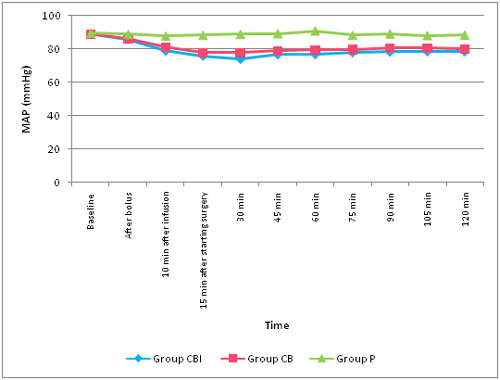
MAP in Group C BI showed significant fall from baseline at all time intervals (p<0.05), whereas in Group CB it was from 10 min after infusion to conclusion of surgery (p<0.05). Maximum fall in MAP was observed at 30 min after starting surgery, and it was 20.45% in Group CBI and 15.38% in Group CB. There was no significant variation from baseline in Group P with respect to MAP (p>0.05). On inter-group comparison, MAP was significantly lower in Group CBI and C B as compared to Group P from administration of bolus dose of study drug to conclusion of surgery(p<0.05). It was significantly lower in Group CBI as compared to GroupC B from 15 min to 105 min of surgery(p<0.05). However, hypotension (SBP < 90 mmHg) was seen in only 2(6.66%) patients of Group C BI (Figure 2).
Fig 2: Comparison of mean arterial pressure (MAP) during intraoperative period
Mean bleeding score was significantly higher in Group P (3.10 ± 0.54) as compared to Group CB (1.36 ± 0.76) and Group CBI (0.86 ± 0.68), (p=0.000). The difference was also significant between Group CB and CBI (p=0.014). Acceptable bleeding score of ≤ 2 was achieved by significantly higher number of patients in Group CBI (n=30, 100%) and Group CB (n=29, 96.67%) as compared to Group P (n=3, 10%), (p=0.000). Group CBI and CB were comparable (p=0.990). Thus incidence of achievement of acceptable bleeding score (≤ 2) was in order ofGroup C BI≈GroupC B>GroupP(Table 2).
Table 2: Comparison of OAAS score, bleeding score, of patient satisfaction score (PSS) and surgeon satisfaction score (SSS)
|
Scores |
Group CBI |
Group CB |
Group P |
P value |
||
|
CBI/CB |
C B/P |
P/CBI |
||||
|
OAAS score |
||||||
|
Mean ± SD |
2.06 ± 0.61 |
2.83 ± 0.70 |
4.80 ± 0.40 |
0.010 |
0.000 |
0.000 |
|
≤ 4 (acceptable) |
30 (100%) |
29(96.67%) |
6 (20.00%) |
0.990 |
0.000 |
0.000 |
|
>4 (unacceptable) |
0 (0%) |
1 (3.33%) |
24(80.00%) |
0.980 |
0.000 |
0.000 |
|
Bleeding score |
||||||
|
Mean ± SD |
0.86 ± 0.68 |
1.36 ± 0.76 |
3.10 ± 0.54 |
0.014 |
0.000 |
0.000 |
|
≤ 2 (acceptable) |
30 (100%) |
29 (96.67%) |
3 (10%) |
0.990 |
0.000 |
0.000 |
|
>2 (unacceptable) |
0 (0%) |
1 (3.33%) |
27 (90%) |
0.950 |
0.000 |
0.000 |
|
PSS |
||||||
|
Mean ± SD |
6.23 ± 0.56 |
5.53 ± 0.49 |
3.80 ± 0.46 |
0.013 |
0.000 |
0.000 |
|
≥ 5 (acceptable) |
30 (100%) |
30 (100%) |
2 (6.67%) |
1.000 |
0.000 |
0.000 |
|
<5 (unacceptable) |
0 (0%) |
0 (%) |
28 (93.33%) |
|
0.000 |
0.000 |
|
SSS |
||||||
|
Mean ± SD |
6.33 ± 0.54 |
5.46 ± 0.50 |
3.86 ± 0.57 |
0.010 |
0.000 |
0.000 |
|
≥ 5 (acceptable) |
30 (100%) |
30 (100%) |
2 (6.67%) |
1.000 |
0.000 |
0.000 |
|
<5 (unacceptable) |
0 (0%) |
0 (%) |
27 (90%) |
|
0.000 |
0.000 |
Patient distribution according to different scores is presented as number (proportion)
All the three Groups were statistically comparable regarding changes in respiratory rate and oxygen saturation at different time intervals intraoperatively (P>0.05).
Table 3: Comparison of rescue sedative and analgesic consumption
|
Scores |
Group CBI |
Group CB |
Group P |
P value |
||
|
CBI/CB |
C B/P |
P/CBI |
||||
|
Rescue sedative requirement |
||||||
|
No. of patients requiring rescue sedative |
1 |
6 |
27 |
0.060 |
0.000 |
0.000 |
|
No. of doses |
1 |
6 |
63 |
0.060 |
0.000 |
0.000 |
|
Mean no. of doses |
0.03 ± 0.18 |
0.20 ± 0.40 |
2.10 ± 1.24 |
0.057 |
0.000 |
0.000 |
|
Rescue analgesic requirement |
||||||
|
No. of patients requiring rescue analgesia |
1 |
6 |
26 |
0.062 |
0.000 |
0.000 |
|
No. of doses |
1 |
6 |
62 |
0.062 |
0.000 |
0.000 |
|
Mean no. of doses |
0.03 ± 0.18 |
0.20 ± 0.40 |
2.07 ± 1.28 |
0.057 |
0.000 |
0.000 |
Acceptable surgeon satisfaction score (SSS) of ≥5 was achieved by all of the patients in Group CBI and CB (n=30, 100%) as compared to only 3 (10%) patients in Group P. The difference was highly significant (p=0.000). Group CBI and CB were comparable regarding incidence of achievement of acceptable SSS (P=1.000). Mean SSS was significantly higher in Group CBI (6.33 ± 0.54) and Group CB (5.46 ± 0.50) as compared to Group P (3.86 ± 0.57), (p=0.000). Mean SSS was significantly higher in Group CBI as compared to Group CB (p=0.010).Acceptable patient satisfaction score (PSS) of ≥5 was achieved by all of the patients in Group CBI and Group CB (n=30, 100%) as compared to only 2 patients (6.67%) in Group P and this difference was highly significant (p=0.000). Group CBI and CB were comparable regarding incidence of achievement of acceptable PSS (P=1.000). Mean PSS was significantly higher in Group CBI (6.23 ± 0.56) and Group CB (5.53 ± 0.49) as compared to Group P (3.80 ± 0.46), (p = 0.000). Mean PSS was significantly higher in Group CBI as compared to Group CB (p = 0.013) (Table 2).
Mean time taken to achieve Aldrete score of 10 was significantly shorter in Group CBI(6.83 ± 2.45)min and Group C B (7.16 ± 2.52)min as compared to GroupP (14.33 ± 3.65)min(p = 0.000), while Group C BI and C B were comparable (p = 0.573).
Adverse effects during the intraoperative period were comparable with no significant difference among the groups (P>0.05). In Group CBI ,a single episode of hypotension (SBP <90 mmHg) was observed in 2 (6.66%) patients and bradycardia (HR <60 /min) in 1 patient (3.33%). In Group P, 2 (6.66%) patients had hypoxia due to supplemental sedative and analgesic drug.
DISCUSSION
Monitored Anesthesia Care (MAC) is a technique where local anesthetics are combined with intravenous sedative drugs for sedation and analgesia. To achieve calm and pain free patient, giving sedative drugs in large doses is the common practice, although the risk of losing airway control, hypoxia and hypotension with higher doses has to be weighed.
MAC may be useful for various ENT surgeries in which, bloodless surgical field is of paramount importance. Bleeding control is usually attained with local application of epinephrine4. Sympathetic stimulation caused by pain during surgery may lead to tachycardia and hypertension and consequently increased bleeding in the surgical field.Commonly used drugs in MAC e.g. benzodiazepines, propofol and opioids have many untoward effects which may hamper patient’s cooperation during surgery and would make these agents less than ideal for the intraoperative management of sedation in MAC.16
With the development of highly specific α2 agonists, clonidine (α2/α1 is 200:1) and dexmedetomidine (α2/α1 is 1600:1), there has been a renewed interest in this class of drugs for use in perioperative period since they offer both sedation, analgesia without significant respiratory depression and can provide induced hypotension with a bloodless surgical field.12
In our study when clonidine was used in MAC; sedation and analgesia were significantly superior as compared to control group. Sedation and analgesic effects of clonidine have been reported in previous studies in which it was used with general anesthesia.11,17,18The locus ceruleus, the largest noradrenergic cell Group in the brain and an important modulator of wakefulness, has been indicated to be the major site for the sedative-hypnotic action of alpha-2 adrenoceptor agonists like clonidine via stimulation of the alpha-2a adrenoceptors.19 The quality of sedation produced by clonidine differs from that of midazolam. Clonidine lacks the psychotropic quality of benzodiazepines and will cause a state of sedation more similar to normal tiredness-sleepiness where the patient can easily be awaken to perform tests. The result is a calm patient who can be easily aroused to full consciousness.20 Clonidine interacts with α-2 adrenoceptors of substantia gelatinosa in the dorsal horn of spinal cord normally responsible for endogenous pain modulation and inhibits the firing of nociceptive neurons stimulated by peripheral A and C fibers.21
In the present study, it was observed that mean arterial pressure and heart rate were significantly lower leading to significantly less bleeding scores in clonidine groups as compared to control groups, which was in concordance to previous studies.12,22,23 Clonidine stimulates α2 adrenergic inhibitory neurons in the medullary vasomotor center resulting in decreased sympathetic nervous system outflow from the central nervous system to the peripheral tissues. It reduces heart rate by a presynaptically mediated inhibition of sympathetic tone caused by a reduction of noradrenaline release, peripheral vasodilatation and by a direct vagomimetic effect.24 Clonidine not only lowers the baseline blood pressure values but also lowers the set point around which arterial blood pressure is regulated. Clonidine neither alters catecholamine metabolism nor does it blocks ganglion transmission or adrenergic receptors. Thus, the protective reflexes triggered by a reduction in blood pressure are still functional and vasoactive and inotropic drugs still remain effective25. Hemodynamic effects of clonidine on intravenous administration occur within 30 min26 approximately which was observed in our study also. Controlled hypotension effectively reduces surgical blood loss and improves surgical conditions. Clonidine facilitates controlled hypotension by decreasing the heart rate, systolic, diastolic and mean blood pressure.27 Clonidine17 and dexmedetomidine14,28 both are found effective in reducing bleeding in ENT surgeries.
Raghuvanshi etal(2014)29 studied the effect of clonidine(30 µg) as an adjuvant with local anesthetic (12 ml of 2% Xylocaine with 1:200000 adrenaline) for in filtration anesthesia in tympanoplasty surgeries. They reported that addition of clonidine to local anesthetic in block was associated with significantly less bleeding in the operative bleeding, improved quality of intraoperative anesthesia and prolonged duration of postoperative analgesia without significant side effects.
We observed that patient and surgeon satisfaction scores were significantly higher in clonidine Groups which could be attributed to superior sedation, analgesia and bloodless surgical field provided by clonidine. Clonidine produces calm patient that can be easily aroused to full consciousness.20 Additional analgesic property of α2 agonists also contributes to higher patient satisfaction rate in clonidine Group. Surgeons were more satisfied in clonidine Group since α2 agonists have the ability to provide bloodless surgical field10,14 and interruption of surgery by patient’s complaint of pain requiring rescue analgesic was also less with clonidine. Many authors have reported better satisfaction profile of patient and surgeon when clonidine was used as adjuvant.12,22
Intravenous clonidine and midazolam were compared for MAC in ENT surgeries in our previous study (Kumari et al 2012).12 Better analgesia, bloodless surgical field and superior satisfaction scores were found in clonidine group, while mean sedation scores were higher in midazolam group. Midazolam causes sedation by GABA receptor activation. Alpha-2 receptors are found densely in the pontine locus ceruleus which is an important source of sympathetic nervous system innervations of the forebrain and a vital modulator of vigilance. The sedation effects evoked by α2 agonists most likely reflects inhibition of this nucleus.12 Results of that study showed that clonidine can’t be an alternative to midazolam in MAC. One more limitation of the study being, clonidine bolus was not followed by infusion.
Taking note of results of previous study, two regimes of clonidine (bolus alone or bolus followed by infusion) were used as an adjunct to conventional MAC regime of midazolam and fentanyl in the present study. When two clonidine regimes were compared,patients receiving clonidine bolus and infusion demonstrated better sedation profile, less bleeding score and higher satisfaction scores as compared to patients receiving clonidine bolus alone.Previous studies12,30 have also recommended that clonidine bolus should be followed by infusion as with dexemeditomidine.6
Despite the sedative properties, clonidine is associated with faster recovery from anesthesia and less postoperative sedation, as it lacks the psychotropic quality and will cause a state of sedation more similar to normal tiredness sleepiness where the patient can easily be awoken20 and also because of the reduced needs for both sedatives as well as opioids. We observed no difference regarding time from the end of surgery to discharge readiness from PACU.
Clonidine in therapeutic doses is devoid of significant adverse effects as supported by our study. Clonidine in higher doses can cause respiratory depression, hypotension and bradycardia.31 It should be avoided in cases of prolonged P-R interval and spontaneous bradycardia. Clinically important complications with clonidine though few, needs to be kept in mind.12
LIMITATIONS
There were certain limitations with the study due to resource constraints at our institute like, inability to measure sedation level with bi spectral index, therapeutic plasma concentrations of clonidine, noradrenaline.
CONCLUSION
We conclude that clonidine 3 µg/kg IV bolus followed by infusion of 0.3 µg/kg/hr may be used as an adjunct to conventional MAC regime of midazolam and fentanyl for variety of ENT procedures. It provides superior sedation, analgesia and bloodless surgical field leading to better satisfaction of both patient and surgeon. Being a safe, well tolerated, cheap and effective regime, our study favors its use in routine for MAC in ENT surgeries.
REFERENCES
- American Society of Anesthesiologists. Standards for Basic Intraoperative Monitoring 1986. Available at: http://www. org/Standards/02.html. (Accessed May 23, 2001)
- Albertin A, Fanelli G. Monitored anaesthesia care. Torino, Ed. UTET; 2001
- Karaaslan K, Yilmaz F, Gulcu N, Colak C, Sereflican M, Kocoglu H. Comparison of dexmedetomidine and midazolam for monitored anesthesia care combined with tramadol via patient-controlled analgesia in endoscopic nasal surgery. Curr Ther Res Clin Exp. 2007 Mar;68(2):69-81.[PubMed][Free full text]doi: 10.1016/j.curtheres.2007.04.001.
- Goksu S, Arik H, Demiryurek S, Mumbuc S, Oner U, Demiryurek AT. Effects of dexmedetomidine infusion in patients undergoing functional endoscopic sinus surgery under local anesthesia. Eur J Anaesthesiol. 2008 ;25(1):22-28.[PubMed]
- Abdellatif AA, Elkabarity RH, Hamdy TAE. Dexmedetomedine vs midazolam sedation in middle ear surgery under local anesthesia: Effect on surgical field and patient satisfaction.Egyptian Journal of Anaesthesia 2012;28:117–123.
- Candiotti KA, Bergese SD,Bokesch PM, Feldman MA, Wisemandle W, Bekker AY. Monitored anesthesia care with dexmedetomidine: a prospective, randomized, double-blind, multicenter trial. AnesthAnalg 2010;110:47–56.[PubMed]doi: 10.1213/ane.0b013e3181ae0856.
- Sarmento KM Jr, Tomita S. Retroauricular tympanoplasty and tympanomastoidectomy under local anesthesia and sedation. Acta Otolaryng 2009;129:726-728.[PubMed]doi: 10.1080/00016480802398996.
- Herr DL, Sum-Ping STJ, England M. ICU sedation after coronary artery bypass graft surgery: dexmedetomidine-based versus propofol-based sedation regimens. J Cardiothorac Vasc Anesth 2003;17:576–84.[PubMed]
- Drown MB. Integrative review utilizing dexmedetomidine as an anesthetic for monitored anesthesia care and regional anesthesia. Nurs Forum 2011;46(3):186-194.[PubMed]doi: 10.1111/j.1744-6198.2011.00229.x.
- Kamibayashi T, Maze M. Clinical uses of alpha2-adrenergic agonists. Anesthesiology 2000;93:1345–1349.[PubMed]
- Jabalameli M, Hashemi SM, Soltani HA, Hashemi SJ. Oral clonidine premedication decreases intraoperative bleeding in patients undergoing endoscopic sinus surgery. J Res Med Sci 2005;10:25-30.
- Kumari I, Naithni U, Bedi V, Gupta S, Gupta R, Bhuie. Comparison of clonidine versus Midazolam in monitored anesthesia care during ENT surgery : A prospective, double blind, randomized clinical study. Anaesth Pain and Intensive Care 2012;16(2):157-64.
- Chernik DA, Gillings D, Laine H, Hendler J, Silver JM, Davidson AB, et al. Validity and reliability of the Observer’s Assessment of Alertness/Sedation Scale: study with intravenous midazolam. J Clin Psychopharmacol 1990;10:244–51.[PubMed]
- Durmus M, But AK, Dogan Z, Yucel A, Miman MC, Ersoy MO. Effect of dexmedetomidine on bleeding during tympanoplasty or septorhinoplasty. Eur J Anaesthesiol. 2007 May;24(5):447-453.[PubMed]
- Aldrete JA. The post-anesthesia recovery score revisited. J Clin Anesth 1995;7:89-91.[PubMed]
- Vyas DA, Hihoriya NH, Gadhavi RA. A comparative study of dexmedetomidine vs midazolam for sedation and hemodynamic changes during tympanoplasty and modified radical mastoidectomy. Int J Basic Clin Pharmacol 2013 Oct;2(5):562-566.
- Maroof M, Khan RM, Bhatti TH. Clonidine premedication for induced hypotension with total intravenous anaesthesia for middle ear microsurgery. Can J Anaesth 1994;41:164-165.[PubMed]
- Stocche RM, Gracia LV, Reis MP, Miranda Junior O. Intravenous clonidine in the induced arterial hypotension technique for tympanoplasty Rev Bcas Anesthesiol 2003;53:457-66.[PubMed]
- Scheinin M, Schwinn D. The locus coeruleus: site of hypnotic actions of alpha-2 adrenoceptor agonists? Anesthesiology 1992;76:873-875.[PubMed]
- Hall JE, Uhrich TD, Ebert TJ. Sedative, analgesic and cognitive effects of clonidine infusions in humans. Br J Anaesth 2001;86(1):5-11.[PubMed]
- Howe JR, Wan J-Y, Yaksh TL. Selective antagonism of the antinociceptive effect of intrathecally applied alpha adrenergic agonists by intrathecal prazosin and intrathecal yohimbine. J Pharmacol Exper Ther 1983;224:552-558. [PubMed]
- Sahoo S, Kaur M, Tripathy HK, Kumar A, Kohli S, Nanda S. Comparative evaluation of midazolam and clonidine as pediatric oral premedication. Anesth Essays Res. 2013 May-Aug;7(2):221-7. [PubMed]doi: 10.4103/0259-1162.118967.
- Lonnquist PA., Bergendahl H. Pharmacokinetic & hemodynamic response after an intravenous bolus injection of clonidine in children. Pediatr Anaesth 1993;3:359-364.
- De Jonge A, Timmermans PBMWM, Van Zwieten PA. Participation of cardiac presynaptic alpha-2 adrenoceptors in the brad ycardic effects of clonidine and analogues. Naunyn Schmiedebergs Arch Pharmacol. 1981 Aug;317(1):8-12.[PubMed]
- Ruffolo RR Jr. Distribution and function of peripheral alpha-2 adrenoceptors on the cardiovascular system. Pharmacol Biochem Behav 1985;22:827-833.[PubMed]
- Eisenach JC, De Kock M, Klimscha W. Alpha-2 adrenergic agonists for regional anesthesia. A clinical review of clonidine (1984-1995). Anesthesiology 1996;85:655-674.[PubMed][Free full text]
- Hackmann T, Friesen M, Allen S, Precious DA. Clonidine facilitates controlled hypotension in adolescent children. Anesth Analg 2003;96:976–81. [PubMed]
- Ayoglu H, Yapakci O, Ugur MB, Uzun L, Altunkaya H, Ozer Y, et al. Effectiveness of dexmedetomidine in reducing bleeding during Septoplasty and tympanoplasty operations. Clin J Anesth 2008;20:437-41.[PubMed] doi: 10.1016/j.jclinane.2008.04.008.
- Raghuvanshi SK, ChakravartyN, Asati DP, Bankwar V. Use of clonidine as an adjuvant to infiltration anaesthesia in tympanoplasty: a randomized double blind study. Indian J Otolaryngol Head Neck Surg 2014;66(1):57-62. [PubMed][Free full text]doi: 10.1007/s12070-013-0664-4.
- Marinangeliaf F, Ciccozzia A, Dontellia F, Di Pietro A,Iovinelli G, Rawal N, et al. Clonidine fortreatment of postoperative pain: A dose finding study. Eur J Pain 2002;6:35-42.[PubMed]
- Nishina K, Mikawa K, Shiga M,Obara H. Clonidine in paediatric anaesthesia. Paediatr Anaesth 1999;9:187-202. [PubMed]
Appendix 1: Various scores used in the study
OAAS score 5—awake and responds readily to name spoken in normal tone.
0 – No bleeding
Score 5,6,7: Acceptable
Total score: 10, score of ≥9 is required for discharge
VAS >3 is pain |
||||||||||||||||||||||||||||||||||||||||
