
Mugdha Markandeya*, Ujjwala Andurkar*, Manisha Sapate*, Rajesh Gore*,
*Consultant in Anesthesiology, Department of Anesthesiology, Yashwantrao Chavan Memorial Hospital, Pimpri, Pune (India)
Correspondence: Dr. Ujjwala S. Andurkar, Yashwantrao Chavan Memorial Hospital, Sant Tukaram Nagar, Pimpri, Pune-18 (India); E-mail: uju_andurkar@yahoo.co.in
ABSTRACT
Some of the main objectives of anesthesia plan for tracheoesophageal fistula (TEF) repair are to provide good analgesia and smooth post-operative recovery. The anesthetic considerations in neonatal surgical emergencies are based on the physiological immaturity of various body systems, poor tolerance to the anesthetic drugs associated with congenital heart disease and preterm baby. The use of regional anesthesia has shown to be safe and effective. TEF repair of 1 day old baby which was successfully managed by caudal epidural analgesia along with GA is reported in this article. So management of every TEF case with caudal block shows excellent hemodynamic stability, postop pain relief for successful recovery and increased survival of the baby.
Key words: Tracheoesophageal fistula; TEF; VSD; Hemivertebra; Caudal epidural; Postoperative analgesia
Citation: Markandeya M, Andurkar U, Sapate M, Gore R. Wonders with caudal epidural analgesia for tracheoesophageal fistula in neonates. Anaesth Pain & Intensive Care 2013;17(2):189-191
INTRODUCTION
Tracheoesophageal fistula (TEF), which manifests in the neonate within the first hours to days of life, is considered a surgically correctable anomaly of the gastrointestinal and respiratory systems. The perioperative anesthetic implications associated with TEF are of acute importance to the anesthesiologist. TEF occurs in about 1 in every 3,000 to 4,500 births and continues to be a major challenge in neonatal surgery. The most frequently associated anomalies with EA±TEF are cardiac (49%) and anorectal malformations (15%).1–4 With surgical repair, the rate of survival exceeds 90%, even in infants with a low birth weight.
CASE REPORT
A 1 day old, 36 week gestational age, 1800 gm infant was delivered at a peripheral hospital. After birth, infant had had laboured breathing due to respiratory distress so he was transferred to our hospital. Baby was admitted in NICU with these clinical findings; heart rate 130/min and RR 52/min without intercostal and subcostal indrawing. On auscultation pansystolic murmur was heard in mitral area. History was positive for having vomited twice on the same day in the evening. Patient was managed with oxygen, nebulisation, antibiotics and CPAP ventilator. Chest x-ray showed TEF test positive (rolling up of NGT) along with presence of hemivertebra at T4 level.
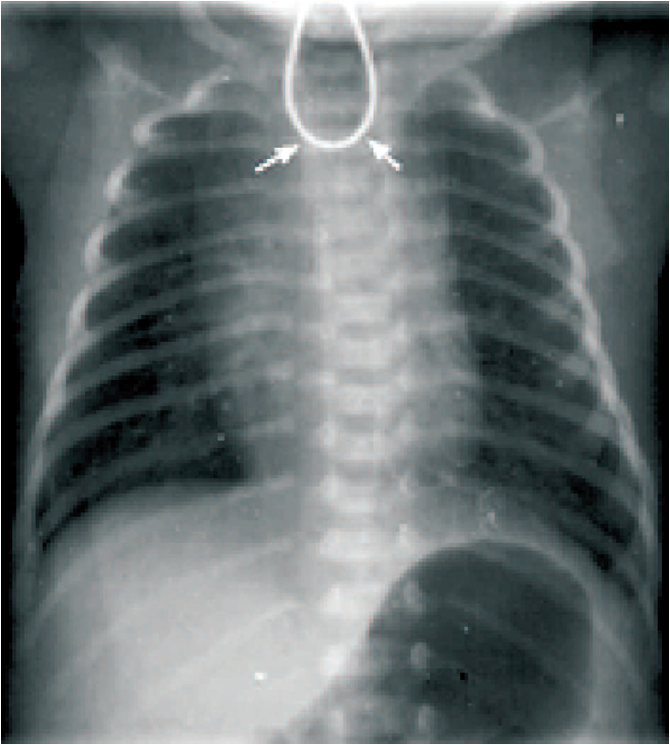
Figure 1: Coiled nasogastric tube in the esophagus
Echocardiography revealed a patent foramen ovale, left to right shunt with 4 mm muscular VSD and mild pulmonary hypertension. Preoperatively baby was managed with nasogastric tube aspiration for excessive secretions two hourly and monitoring of oxygen saturation. Patient was diagnosed as a case of tracheoesophageal fistula type IIIB. After stabilization and preoperative evaluation patient was accepted for surgical repair of TEF under ASA-III E. GA along with caudal epidural was planned for surgery. Laboratory investigations were within normal limits. Preoperatively patient was adequately hydrated with intravenous fluids 60 ml/kg/day, with nasogastric tube in situ. The risks to the life were explained to the parents, a high-risk consent was taken along with adequate arrangements at NICU including neonatal ventilator and PCV. Patient was transferred to the operating room with oxygen hood (5-6 lit/min).
In the operating room, after securing an intravenous line with 24G cannula, monitors were attached for SpO2, ECG and heart rate. Precordial stethoscope was fixed in mitral area. Care of hypothermia was taken by wrapping the baby with cotton rolls and silver foils. Nasogastric aspiration was done with 2 ml syringe. Baby was premedicated with inj. glycopyrrolate 0.004 mg/kg, fentany l0.5 µg/kg, midazolam 0.01 mg/kg, ondensetron 0.1 mg/kg, hydrocortisone 5 mg/kg and dexamethasone 1 mg/kg.
Preoxygenation was done for 5 min with 100% oxygen. Baby was induced with inj. ketamine 2 mg/kg IV along with sevoflurane 1.5%. Baby was intubated in deep plane of anesthesia without muscle relaxant and intubation was done with Portex™ uncuffed ETT No. 2.5 under direct vision. Tube was located below the level of TEF but above the carina and taped after confirming bilateral air entry. Patient was maintained on assisted spontaneous ventilation with oxygen and sevoflurane 0.4% on Jackson-Rees pediatric circuit. She was placed in lateral position and under aseptic precautions, an epidural catheter with bacterial filter was placed in the caudal space and advanced upto T4 level i.e. upto 12cm from the surface of the skin. Confirmation was done by meniscus test and the catheter was fixed. Inj bupivacaine 0.25% in the dose of 0.5 mg/kg was used. Patient was then handed over to the surgeons.
Intraoperatively, fluid management was done according to 4/2/1rule i.e. 50 ml of pediatric electrolyte solution (Kidral-P™). Heart rate was kept between 130-140/min. SpO2, ECG and urine output were continuously monitored. Blood loss was replaced in the ratio of 1:1. Suddenly there was a fall in SpO2, air entry was checked and found to be absent. Hence patient was made supine anticipating ETT blockage. The tube was replaced and SpO2 improved. Intercostal chest drainage was placed and column movement was seen
Postoperatively, patient was extubated after assessing the muscle tone, blast and respiration. Epidural analgesia with inj. bupivacaine 0.25% 0.5 mg/kg was again via repeat boluses. Paracetamol suppository was inserted and the patient was shifted to NICU for postoperative management. Epidural top-up dose for analgesia was titrated according to hemodynamic parameters. There was no tachycardia or tachypnea and the baby was comfortable. Epidural catheter was removed after 48 hrs and feeds were started on sixth postop day. Breast feeding was started on ninth postop day.
DISCUSSION
Well known classification system describes 5 types of TEF; types I, II, IIIA, IIIB, and IIIC.1 Regardless of the classification, the most common form of this anomaly is esophageal atresia (EA) with distal TEF. Our patient belonged to the category of IIIB. EA is usually diagnosed shortly after birth if a nasogastric tube cannot be passed beyond 8 to 10 cm. The diagnosis is further confirmed by a chest X-ray showing a nasogastric tube curled in the upper chest or neck region. Infants with TEF are premature and they have high incidence of congenital heart disease and other anomalies. The most frequently associated anomalies with EA±TEF are cardiac (49%) and anorectal malformations (15%).1–4 This baby had VSD as well as hemivertebra (T4) which are the components of VACTERL anomalies.5 Patient had increased salivation and tachypnea hence she was kept in semi-upright position with a catheter in the blind pouch with low suction.
The main principles of anesthetic management include assessment of the special anesthetic problems associated with TEF. Associated anomalies like VSD and hemivertebra were listed. Identification of main pathophysiology associated with TEF was done. Anesthetic plan i.e. awake intubation, spontaneous ventilation, fluid and electrolyte management was decided. Plan for intra-op and postop analgesia was also considered. Before induction, pouch was aspirated and patient was induced with inhalational agents and intubated deep without muscle relaxants. Caudal epidural catheter was inserted and kept in situ upto 48 hours postoperatively.6 Infants, smaller than 2 kg, may require postoperative mechanical ventilation or reintubation if the patient is extubated, but with caudal epidural analgesia, recovery is good. In a recent study conducted by Al-Mendalawi et al., mortality rate in TEF is maximum due to respiratory failure and sepsis and is the least due to cardiac arrest during anesthesia.7 Bosenberg et al. found that for EA surgery, caudal epidural anesthesia reduces the need of postoperative ventilatory support.8 Kinottenbelt G et al showed that a caudal catheter can be advanced to T6-T7 to supplement the general anesthesia and provide excellent postop analgesia without the use of opioids and to facilitate extubation.9 Atzori P et al. suggested that tracheobronchoscopy is a useful and safe procedure and should be recommended in tertiary centres for babies with EA before surgical repair.10
Post-operative considerations:
Usually postoperative ventilatory support is required in TEF surgery, but in our case it was possible to extubate the baby on table because of caudal epidural analgesia which was provided for 48 hours post operative. Postop infection was taken care of. A follow up barium meal x-ray showed no leak and the baby was discharged in a healthy condition.
CONCLUSION
As there are many complex factors involved, anesthetic management for surgical repair of TEF is based on individual experience and confidence in handling the case. Decision in planning of anesthesia and good foundation in physiological and pharmacological principles will surely contribute to successful outcome and good survival rate. Caudal epidural analgesia may be employed usefully with general anesthesia in neonates.
REFERENCES
1. Spitz L. Esophageal Replacement. In: Grosfeld JL, O’Neill JA Jr, Coran AG, Fonkalsrud EW, editors. Pediatric Surgery. 6th ed. Philadelphia PA: Mosby Elsevier; 2006. pp. 1093–106.
2. Shaw-Smith C. Oesophageal atresia, tracheo-oesophageal fistula, and the VACTERL association: Review of genetics and epidemiology. J Med Genet. 2006;43:545–54. [PMC free article] [PubMed]
3. Depaepe A, Dolk H, Lechat MF. The epidemiology of tracheo-oesophageal fistula and oesophageal atresia in Europe. Arch Dis Child. 1993;68:743–8. [PMC free article] [PubMed]
4. Chittmittrapap S, Spitz L, Kiely EM, Brereton RJ. Oesophageal atresia and associated anomalies. Arch Dis Child. 1989;64:364–8. [PMC free article] [PubMed]
5. Gayle JA, Gomez SL. Preanesthetic assesment of the neonate with tracheoesophageal fistula. Lesson 273, Anesthesiologynews.com April 2008;43-46.
6. Bricker SR, Telford RJ, Booker PD. Pharmacokinetics of bupivacaine following intraoperative nerve blocks in neonates and infants less than 6 months. Anesthesiology 1989 Jun;70(6):942-7. [PubMed] [Free Full Text]
7. Al Mendalawi MD, Jabbar Al-Rudaini MA, JABHS 2012;13:(ISSN 1561-0217), available from: http://www.arab-board.org [Last accessed on 2012 Aug 15].
8. Bosenberg AT, Hadley GP, Wiersma R. Esophageal atresia: Caudo-thoracic epidural anesthesia reduces the need for post-operative ventilator support. Pediatr Surg Int 1992;7:289-91. [Access Online]
9. Kinottenbelt G, Skinner A, Seefelder C. Tracheo-esophageal fistula(TOF) and oesophageal atresia(OA). Best Pract Res Clin Anesthesiol 2010;24:387-401. [PubMed]
10. Atzori P, Iacobelli BD, Bottero S, Spirydakis J, Laviani R, Trucchi A, et al. Preoperative tracheobronchoscopy in newborns with esophageal atresia: Does it matter? J Pediatr Surg 2006;41:1054-7. [PubMed]
