
Asoka Gunaratne, MBBS, MD, FCARCSI*
*Consultant Anaesthetist, Teaching Hospital, Karapitiya, Galle (Sri Lanka)
Correspondence: Asoka Gunaratne, Consultant Anaesthetist, Teaching Hospital, Karapitiya, Galle (Sri Lanka)
ABSTRACT
Acute superior vena cava obstruction is commonly benign and often due to thrombosis following central venous catheterization or placement of pace maker wires. Acute obstruction due to malignancy is rare. We report a young patient known to have a malignant anterior mediastinal tumor developing acute SVC obstruction causing total airway obstruction in the anaesthetic recovery room following surgery unrelated to the mediastinum.
Key words: Superior vena cava; Mediastinal tumor
Citation: Gunaratne A. Acute superior vena cava obstruction causing total airway obstruction in the anaesthetic recovery room. Anaesth Pain & Intensive Care 2009;13(1):25-27
INTRODUCTION
Majority of cases of acute onset superior vena cava (SVC) obstruction is due to thrombosis caused by central venous catheters1. Most other causes of acute obstruction are benign. Malignancies generally cause a gradual obstruction and the commonest of these is bronchogenic carcinoma2. Lymphoma and thymoma are the other main non benign causes. However, acute onset obstruction is rare in these patients.
CASE REPORT
A 29-year-old male patient with neurofibromatosis presented with a painful neurofibroma at the back of the chest. He had had a similar painful neurofibroma at the right elbow which was surgically excised earlier. The histology of it was reported as a neurofibroma undergoing malignant transformation. The patient was also known to have a malignant mediastinal tumor. This had been an incidental finding in a routine chest x-ray done in a medical unit where the patient had presented with a persistent cough (Fig 1). Subsequently a CT of the chest was performed and a tumor in the anterior mediastinum was confirmed (Fig 2). The histology of the CT guided biopsy revealed a malignant epithelial peripheral nerve sheet tumor. He was treated with four cycles of chemotherapy by the oncologist. A biopsy taken from the painful neurofibroma of the current presentation once again revealed a neurofibroma undergoing malignant transformation. A palliative wide local excision of the lesion was planned.
Figure 1: Mediastinal tumour on plain x-ray chest
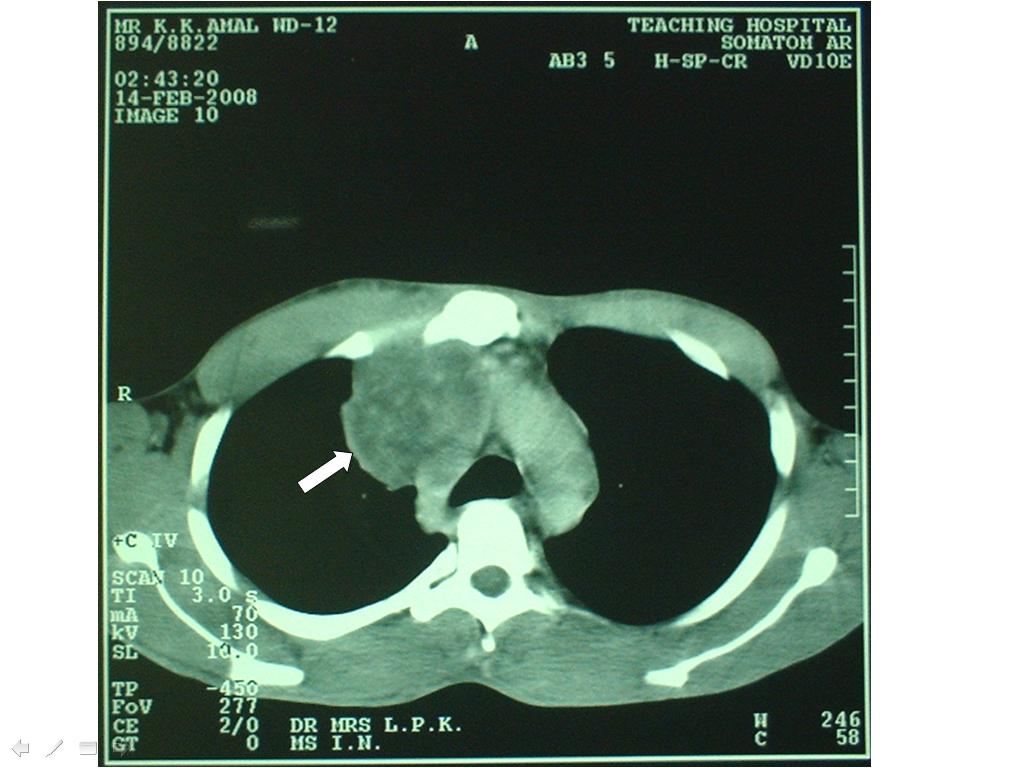
Figure 2: CT scan of the chest of the same patient. White arrow shown mediastinal tumour
The patient had a general anaesthetic for his surgery which was uneventful. At the recovery following surgery, he became acutely short of breath. His face and the neck started to swell rapidly and the oxygen saturation dropped. As he could not be ventilated with the mask, a decision was made to intubate him. However, all attempts at intubation failed and the patient suffered a respiratory arrest. An emergency percutaneous mini tracheostomy attempted at this stage was successful. As the patient could now be ventilated, he was taken back to the operating room where the surgeon performed a formal tracheostomy. The patient was then transferred to the intensive care unit (ICU) for ventilation. He was reviewed by the oncologist again and was treated with radiotherapy. During the cause of his treatment the swelling of the face and neck completely disappeared. He was spontaneously breathing through the tracheostomy which was still in situ. Decannulation was done three weeks later before his discharge from the ICU.
DISCUSSION
SVC obstruction is a serious condition which can be caused by a benign or malignant disease. In one case series malignancy was by far the most common etiology2. The most frequent malignancies are bronchial carcinoma followed by non-Hodgkin lymphoma. Benign lesions are usually reported due to thrombosis related to central venous catheters1. It has also been reported due to other causes such as a primary tumor of the SVC, rupture of a bronchial or innominate artery, aneurysm or aortic dissection. Essentially any mediastinal mass may compress or invade the SVC.
With slowly progressive obstruction of the SVC, adequate collaterals may develop. In acute obstruction there is no time for their development and symptoms develop rapidly. The most common symptoms are facial and neck swelling, bilateral upper extremity swelling, headache and shortness of breath.
In the assessment of the patient the presence or the absence of venous thrombosis must be determined. Ultrasonography is useful for excluding thrombosis. If the SVC cannot be directly imaged its patency may be indirectly determined with normal wave forms in the subclavian and brachiocephalic veins. In patients with a suspected mediastinal mass CT of the thorax should be performed3. Obtaining a tissue diagnosis by means of a percutaneous biopsy under CT guidance is the first step in the treatment of patients with SVC syndrome caused by a mediastinal mass. Patients with malignant obstruction of the SVC have a short life expectancy. The goal in treating these patients is to provide relief of symptoms. Surgical treatment in this patient population is extremely limited. Radiation or chemotherapy is the main mode of treatment. The decision to use either or both is made on the basis of histological characteristics of the tumor. Patients have improved with both modalities with response rates greater than 70%4. SVC stents have been used in patients in whom the condition failed to respond to traditional therapy or in whom symptoms recurred after such therapy. Relief of symptoms has been demonstrated in more than 90% of patients with stents5, 6.
Patients with a benign lesion often have a normal life expectancy and are treated with angioplasty or stent placement. Long term patency of SVC stents has not been proved. Surgical bypass of the SVC obstruction is extremely invasive and requires a high level of expertise, however, good patency rates have been reported7. Those with central venous thrombosis should receive anticoagulation for 3-6 months because they can have significant pulmonary embolization. A timely diagnosis and appropriate treatment will result in a favorable outcome.
REFERENCES
- Qanadli SD, Mesurolle B, Sissakian JF, Chagnon s, Lacombe P. Implanted central venous catheter related acute superior vena cava syndrome: management by metallic stent and endovascular repositioning of the catheter tip. Eur Radiol 2000;10:1329-31. [Medline]
- Chen JC, Bongard F, Klein SR. A contemporary perspective on superior vena cava syndrome. Am J Surg 1990;160(2):207-11. [Medline]
- Schwartz EE, Goodman LR, Haskin ME. Role of CT scanning in the superior vena cava syndrome. Am J Clin Oncol 1986;9(1):71-8. [Medline]
- Armstrong BA, Perez CA, Simpson JR. Role of irradiation in the management of superior vena cava syndrome. Int J Radiat Oncol Biol Phys 1987;13(4):531-9. [Medline]
- Dyet JF, Nicholson AA, Cook AM. The use of the wall stent endovascular prosthesis in the treatment of malignant obstruction of the superior vena cava. Clin Radiol 1993;48(6):381-5. [Medline]
- Tanigawa N, Sawada S, Mishima K, Okuda Y, Mizukawa K, Ohmura N, et al. Clinical outcome of stenting in superior vena cava syndrome associated with malignant tumors. Comparison with conventional treatment. Acta Radiol 1998;39(6):669-74. [Medline]
- Doty JR, Flores JH, Doty DB. Superior vena cava obstruction: by pass using spiral vein graft. Ann Thorac Surg 1999;67(4):1111-16. [Medline]
