
Dinesh Singh, DNB1, Ajay Kumar, MD2, Misha Sethi, MD3
1Ex-Senior Resident; 2Specialist; 3Ex-Junior Specialist,
Department of Anaesthesiology & Critical Care, Deen Dayal Upadhyay Hospital, New Delhi, India- 110064
Correspondence: Dr. Ajay Kumar, BB/49-C, Janakpuri, New Delhi, (India) – 110058; Phone: 9818494758; E-mail: ajayannu@gmail.com
ABSTRACT
Background and Aims: To study and compare the time taken, success and ease of awake tracheal intubation using lightwand-guided ILMA and LMA CTrachTM after application of manual in-line stabilization, in adult patients with simulated cervical spine injury.
Methodology: Eighty adult patients were randomized into two groups. In ILMA–LW group trachea was intubated using lightwand-guided ILMA and in LMA CTrachTM group using CTrachTM LMA. After anesthetizing patient’s airway with topical local anesthetic, manual in-line stabilization was applied by an assistant, study device was inserted and trachea was intubated through it. The time taken, success and ease of tracheal intubation was noted. The observations of the study were compiled and analyzed statistically. Fischer´s exact test and Chi-square test were used for qualitative data. Quantitative data within groups was analyzed using paired t-test and non-parametric Wilcoxon signed rank test and for quantitative data between groups, Student´s t-test and Wilcoxon Mann Whitney test was used. The level of statistical significance was taken as p < 0.05.
Results: The mean time required for tracheal intubation was 47.86 ± 11.76 sec in ILMA–LW group as compared to 64.84 ± 15.97 sec in LMA CTrachTM group (p < 0.001). Success of tracheal intubation was 87.5% and 80% in group ILMA-LW and group LMA CTrachTM respectively (p = 0.363). Ease of intubation, number of adjusting maneuvers and intubation attempts, hemodynamic parameters, post-operative oropharyngolaryngeal morbidity and patient’s experience of the procedure were comparable between the two groups.
Conclusion: In patients with simulated cervical spine injury after application of manual in-line stabilization, awake tracheal intubation through lightwand-guided ILMA (ILMA-LW) was significantly faster than LMA CTrachTM with comparable success and ease of intubation.
Key words: Intubation, Endotracheal; Awake intubation; Lightwand-guided ILMA; LMA CTrachTM
Citation: Singh D, Kumar A, Sethi M. Awake intubation using lightwand-guided ILMA versus LMA CTrach in patients with simulated cervical spine injury. Anaesth Pain & Intensive Care 2016;20(4):439-446
Received: 10 Jul 2016; Reviewed: 18, 25 Nov, 5 Dec 2016; Corrected: 30 Nov 2016; Accepted: 12 Dec 2016
INTRODUCTION
Airway management in patients with cervical spine injury presents a challenge to the anesthesiologist. These patients may require immediate control of airway or may later present for elective surgical procedures. Awake intubation in patients with cervical spine injury is safe and does not cause neurological deterioration.1 The splinting action of normal cervical muscle tone, in awake patients is protective.2
In patients of blunt trauma, the incidence of cervical spine injury has been reported as two to five percent.2Airway maneuvering during laryngoscopy may cause significant movement at the cervical spine and aggravate the injury, necessitating the need to avoid or minimize this movement. Manual in line stabilization provided by an assistant reduces the cervical spine movement during laryngoscopy but increases the difficulty in visualizing the larynx.
The Intubating Laryngeal Mask Airway (ILMA) and LMA CTrachTM can be inserted in neutral position of head and neck and facilitate intubation in these patients.3,4 ILMA can be used for guided tracheal intubation either blindly or using visualizing techniques like fibreoptic bronchoscope or lightwand. LMA CTrachTM is a modification of ILMA with a fibreoptic system and a detachable LCD viewer. This system enables real time viewing of the glottis to guide tracheal intubation via laryngeal mask conduit.
To the best of our knowledge, awake intubation through ILMA-LW and LMA CTrachTM, has not been compared in patients with simulated cervical spine injury. Hence, we undertook this study to compare these two devices for awake tracheal intubation in patients with simulated cervical spine injury with application of manual in line stabilization.
Hypothesis: The study hypothesis is that LMA CTrachTM , which enables real time viewing of the glottis to guide tracheal intubation via laryngeal mask conduit, should result in faster tracheal intubation with a greater success and ease as compared to ILMA-LW.
METHODOLOGY
We conducted this prospective, randomized study, over a period of one year, in 80 adult patients, after obtaining approval of the institutional ethical committee and informed consent.
Patients in the age group 18 to 60 years, of either gender, belonging to ASA physical status I or II, scheduled for elective surgical procedure requiring general anesthesia with oro-tracheal intubation were included in the study. Exclusion criteria included patient’s refusal, risk of aspiration, known sensitivity to lignocaine, weight < 30 kg, mouth opening < 2.5 cm, oropharyngeal pathology, surgery of oropharynx or larynx and surgical procedures greater than two hours duration.
Patients were randomly allocated using computer generated random number table to either group ILMA–LW (n = 40), when tracheal tube (ETT) was inserted using lightwand-guided ILMA or group LMA CTrachTM (n = 40), when ETT was inserted through LMA CTrachTM. Concealment of allocation was done using sequentially numbered, opaque, sealed envelopes, that were numbered in advance, opened sequentially, after the participant’s name and other details were written on the appropriate envelope. The study device was inserted by the same anesthesiologist, who had successfully intubated the trachea in more than twenty patients using each of the two devices.
Size of the ILMA (Laryngeal Mask Company, Singapore) or LMA CTrachTM (Laryngeal Mask Company, Singapore) was selected as per the manufacturer’s recommendation (size 3, 4 and 5 for weight of patient 30 to 50 kg, 50 to 70 kg and > 70 kg respectively). Silicone wire reinforced cuffed ILMA ETT size 7 mm for female and size 8 mm for male patients was used for the initial attempt. After selecting the appropriate sized ILMA or LMA CTrachTM, the ILMA ETT was lubricated and tested whether it passed to and fro through the shaft of the mask. Lightwand used in this study was TrachlightTM (Laerdal Medical AS, Tanke Svilandsgate Stavanger, Norway).
In the ILMA-LW group, lightwand (without its metal stylet) was lubricated and inserted into the ETT, with its tip positioned just at the bevel of the tube. This whole assembly was then loaded into the ILMA with the tip of the assembly just at the epiglottis elevating bar, the transverse marking on the ETT (at 15 cm) also acting as a guide to the final position of the assembly. This fully loaded gadget was the study device for group ILMA-LW. For group LMA CTrachTM, antifog solution was applied to the lens and a well lubricated ETT was loaded into LMA CTrachTM, with the tip of the ETT just at the epiglottic elevating bar. This was the study device for group LMA CTrachTM. Modified grip was used in both the groups where index finger was used to stabilize the gadget, as shown in Figure 1 and 2. The tip of the posterior surface of both the devices was lubricated using Lubic jelly (Neon Laboratories Limited, Mumbai, India).
Patients were kept fasting overnight and pre-medicated with tab alprazolam 0.25 mg and tab ranitidine 150 mg on the night before and two hours prior to surgery. Pre-operatively Mallampati class, mouth opening and thyromental distance were noted. Intramuscular glycopyrrolate (0.2 mg) was administered 45 minutes before the procedure. Patient’s airway was anesthetized topically with 2% lignocaine viscous gargles, 10% lignocaine spray and 4% topical lignocaine using ultrasonic nebulizer. In the operating theater, standard monitors (electrocardiogram, non-invasive blood pressure, pulse oximeter) were applied. Fentanyl 2 µg/kg and midazolam 0.03 mg/kg were given intravenously. With head in neutral position, manual in-line stabilization (MILS) was provided by another anesthesiologist, who stood beside the patient in front of the intubator, with hands placed on the sides of the patient’s head and forearms resting on the patient’s chest. The same anesthesiologist applied MILS in all patients. Patient was asked to open his mouth and protrude the tongue; thereafter the study device was inserted and its cuff inflated with recommended volume of air.
In group ILMA-LW, after reducing room lighting, lightwand with pre-loaded ETT was advanced while observing the glow in the neck. A bright glow in the midline at the level of laryngeal prominence, that continued with the downward movement and disappeared at the level of suprasternal notch, indicated correct placement of ETT in the trachea. Adjusting maneuvers,5 (Table 1) were performed, if glow was not visualized in midline or resistance was felt during insertion of ETT. After tracheal intubation, the lightwand was removed and tracheal intubation confirmed by capnography. Auscultation of bilateral lung fields was done. ILMA was removed using a stabilizer rod.
Table 1: Maneuvers performed in ILMA-LW group, to facilitate ETT insertion, depending on position of glow in the neck
| Glow Position | Maneuvers performed |
| Midline (above laryngeal prominence) | ILMA handle flexion; extension; up-down maneuver; try smaller size ETT |
| Midline (below laryngeal prominence) | ILMA handle is withdrawn partially; extended; withdrawn partially and extended |
| Lateral (right or left) | ILMA handle is twisted |
| No glow | ILMA handle is withdrawn partially and extended; check the bulb |
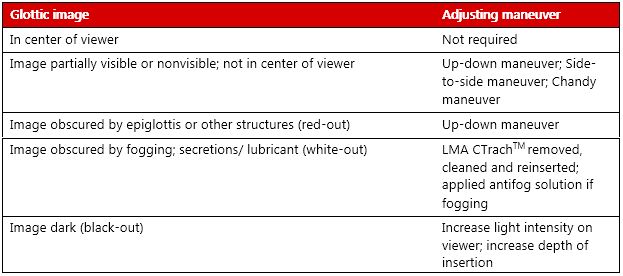
In group LMA CTrachTM, we attached a fully charged viewer to LMA CTrachTM. If the glottis was visible in the center of the screen, the ETT was inserted into the glottic aperture under vision. If a centralized glottic image was not seen, adjusting maneuvers6-10 (Table 2) were performed. ETT was inserted and confirmed by capnography. Auscultation of bilateral lung fields was done. LMA CTrachTM was subsequently removed using a stabilizer rod.
Table 2: Adjusting maneuvers performed in group LMA CTrachTM to obtain a centralized glottic image on the viewer
During insertion of any of the devices, if patient had gagging or complained of discomfort (demonstrated by raising his right hand as instructed), the device was withdrawn and reinserted after optimizing sedation and/or topical anesthesia. Maximum of two trials of optimization were done.
If the patient was not co-operative even after optimization of topical anesthesia/sedation or SpO2 fell below 90% or there was more than 30% change in baseline parameters; the procedure was abandoned. The trachea was intubated using Macintosh laryngoscope after induction of general anesthesia and the case was excluded from the study.
We allowed a maximum of two attempts for study device insertion, four attempts for study device maneuvering and five attempts for ETT insertion. If these attempts were exhausted or tracheal intubation was not achieved within 120 sec, general anesthesia was induced and trachea was intubated using Macintosh laryngoscope. These cases were taken as failed intubation.
After successful intubation, the ease of intubation was rated on a VAS score of zero to ten (ten being easiest). The time required for tracheal intubation was defined as the time from the device entering between the incisors to the time when tracheal intubation was confirmed by capnograph tracing. An intubation attempt was defined as forward or backward movement of ETT through the ILMA or LMA CTrachTM for intubation of trachea.
Failed intubation was defined as intubation achieved after exhaustion of allowable time or number of attempts. In case of esophageal intubation, if the number of attempts had not exhausted, the ETT was withdrawn till the epiglottic elevating bar and reinserted.
Vital parameters such as pulse rate, blood pressure and SpO2 were noted before and after insertion of the device and every minute till five minutes post-intubation. Post-operatively, an independent observer blinded to the method of intubation assessed oro-pharyngo-laryngeal morbidity at 24 hours, trauma to lips, oral mucosa or dental injury and patient’s experience during the procedure.
Statistical Analysis: The observations of the study were compiled and analyzed statistically. Fischer´s exact test and chi-square test were used for qualitative data. Quantitative data within groups was analyzed using paired t-test and non-parametric Wilcoxon signed rank test and for quantitative data between groups, Student´s t-test and Wilcoxon Mann Whitney test was used. The level of statistical significance was taken as p < 0.05. The sample size was estimated as 40 in each group, to detect an assumed difference of 60s between the two groups from the effect size of 0.65 with alpha error of 0.05 and power 80%.
RESULTS
The patient characteristics such as age, gender, ASA class, weight, height, body mass index, Mallampati class, mouth opening and thyromental distance were comparable in both the study groups (Table 3). Hemodynamic parameters were comparable between the two groups. In both the groups none of the patients had desaturation.
Study device insertion was successful at first attempt in all 40 patients in ILMA-LW group as compared to 37 patients in LMA CTrachTM group. Three patients in group LMA CTrachTM required two insertion attempts (Table 4). Number of adjusting maneuvres required in both groups was as depicted in Table 4. Adjusting maneuvres were not required in 14 patients of each group.
The number of intubation attempts required was comparable between the two groups (Table 4). Intubation was successful in first attempt in 24 (60%) and 22 (55%) patients in ILMA-LW and LMA CTrachTM groups respectively. Tracheal intubation was significantly faster in ILMA-LW group with mean time required for tracheal intubation being 47.86 ± 11.76 sec as compared to 64.84 ± 15.97 sec in LMA CTrachTM group (p < 0.001).
Success of tracheal intubation was statistically comparable between the two groups (Table 4). Intubation was successful in 35 of 40 (87.5%) patients in group ILMA-LW and in 32 of 40 (80%) patients in LMA CTrachTM group. Ease of intubation was similar between the two groups with p value being 0.809 (Table 4).
Oro-pharyngo-laryngeal morbidity in form of sore throat and hoarseness was comparable between the two groups. None of the patients in either group had dental injury. However, lip and mucosal injuries were noted in one (2.5%) and six (15%) patients in ILMA-LW and three (7.5%) and four (10%) patients in LMA CTrachTM group respectively.
Regarding patient’s experience of the procedure, 20 (50%) patients in each group had ‘no recall’ of the procedure. Nineteen (47.5%) and 17 (42.5%) patients in ILMA-LW and LMA CTrachTM groups respectively, did not find the procedure unpleasant. While, one (2.5%) and two patients (5%) in ILMA-LW and LMA CTrachTM groups respectively found the procedure ‘unpleasant’. One patient (2.5%) in the LMA CTrachTM group found the procedure to be distressing.
Table 3: Characteristics of patients in ILMA-LW and LMA CTrachTM groups. Values are expressed as Mean (SD) or number (proportion).
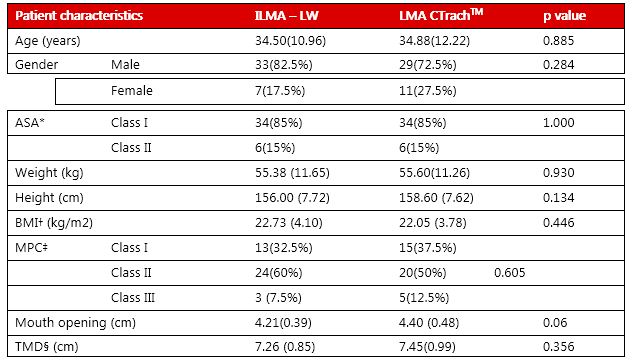
Table 4: Comparative intubation characteristics in ILMA-LW and LMA CTrachTM groups. Values are expressed as median (IQR [range]) or n (%).
| ILMA – LW
( n = 40) |
LMA CTrachTM
( n = 40) |
p value | ||
| Insertion attempts of
study device 1/2 |
40(100)/0 | 37(92.5)/3(7.5) | 0.241 | |
| Number of
adjusting maneuvers |
0 | 14(35) | 14(35) | 0.833 |
| 1 | 8(20) | 7(17.5) | ||
| 2 | 9(22.5) | 6(15) | ||
| ≥ 3 | 9(22.5) | 13(32.5) | ||
| Number of intubation attempts | 1 | 24(60) | 22(55) | 0.884 |
| 2 | 6(15) | 7(17.5) | ||
| 3 | 6(15) | 6(15) | ||
| ≥ 4 | 4(10) | 5(12.5) | ||
| Successful intubation | 35(87.5) | 32(80) | 0.363 | |
| Time required for intubation (s) | 47.86 ± 11.76 | 64.84 ± 15.97 | < 0.001 | |
| Ease of intubation (VAS score) | 8 [7-9(0-10)] | 8 [7-9(0-10)] | 0.809 | |
| Complications (injury)
|
Lip | 1(2.5) | 3(7.5) | 0.172 |
| Mucosal | 6(15) | 4(10) | ||
| Dental | 0(0) | 0(0) | ||
|
Patient’s experience of the procedure |
1-no recall | 20(50) | 20(50) |
0.695 |
| 2-not unpleasant | 19(47.5) | 17(42.5) | ||
| 3- unpleasant, | 1(2.5) | 2(5) | ||
| 4-distressing | 0(0) | 1(2.5) | ||
DISCUSSION:
Awake tracheal intubation in patients with cervical spine injury permits neurological monitoring2 and examination following the intubation procedure. This may be important from a medico legal point of view, as it can be documented that no new neurological deficit has occurred due to the procedure. The cervical muscle tone is protective,2 and awake patients can maintain their airway and respiration adding to the safety. A fiberscope may be used for awake tracheal intubation but this may not always be available. Both devices, LMA CTrachTM and ILMA can be introduced in neutral position of head and neck.3,4 They may be used to facilitate tracheal intubation in patients with cervical spine injury, in whom movement at cervical spine is not desirous.
This study describes the performance of ILMA-LW and LMA CTrachTM for awake tracheal intubation in patients with simulated cervical spine injury after application of MILS. The ILMA-LW could be successfully inserted in all 40 (100%) patients in the first attempt. Other authors have also observed similar results in placement of ILMA.11-15 We could successfully insert the LMA CTrachTM in the first attempt in 37 of 40 (92.5%) patients. Three patients required two insertion attempts. One of these patients’ had gagging and required optimization of topical anesthesia. While, excessive secretions had required device removal and reinsertion after cleaning, in other two patients. Lopez et al. in their study on awake intubation in patients with difficult airway using the LMA CTrachTM found 95% success rate at first attempt placement of LMA CTrachTM.8 Supplemental sedation and topical anesthesia was required to facilitate insertion in one of their patients. Some authors have reported 100% successful insertion of LMA CTrachTM in first attempt.15-18 However, these studies were conducted in anesthetized patients. Patient preparation and co-operation plays an important role in successful placement of a device in awake patients.
We needed to perform one or more adjusting maneuvers in 26 of 40 (65%) patients in both ILMA-LW and LMA CTrachTM groups (Table 4). Lopez et al. performed corrective maneuvers in 12 of 21 (57.14%) patients undergoing awake intubation through LMA CTrachTM.8 Liu et al. applied optimization maneuvers with LMA CTrachTM in (97 of 134) 72.4% patients.19 However, some authors have reported requirement of optimization maneuvers with LMA CTrachTM in lesser number of patients.20 Dimitriou et al. required adjusting maneuvers in 45.45% (20 of 44 ) cases of lightwand-guided tracheal intubation via ILMA.21 As compared to the conventional blind intubation through ILMA, light-guided intubation required fewer adjusting maneuvers.5,12
Our success rate of tracheal intubation was 87.5% (35 of 40) in ILMA-LW group. Of the five subjects in whom tracheal intubation was considered a failure, in two patients number of attempts in device maneuvering had exhausted, while in three patients the allowed time limit had elapsed. Asai et al. also successfully performed light-guided tracheal intubation through ILMA in 9 of 10 (90%) patients.22 A higher success rate has been reported by some authors.21 Kihara et al.12 and Dimitriou and Voyagis5 have reported 100% success in light wand-guided tracheal intubation via ILMA.
We found 80% (32 of 40) success rate of tracheal intubation through LMA CTrachTM . Tracheal intubation failed in eight subjects. In two patients number of attempts for device maneuvering had exhausted, in five patients the allowed time had elapsed and in one patient both number of allowed maneuvers and time limit were exceeded. Malik et al. observed 90% success rate in tracheal intubation with LMA CTrachTM.9 While, some authors have reported 100% intubation success rate through LMA CTrachTM .15,17,19,20 In our study, the success of tracheal intubation was comparable (p = 0.363) between ILMA-LW (87.5%) and LMA CTrachTM (80%) groups. Most of the previous studies involving ILMA-LW or LMA CTrachTM have recorded higher intubation success than ours, probably because these were performed in paralyzed patients as against awake patients in our study. In a paralyzed patient, placement of the device and maneuvering is easier. In awake patients more resistance is encountered due to tone of pharyngeal muscles and maneuvers done at the handle may not get fully transmitted to the mask. The results obtained in paralyzed patients may not apply to non-paralyzed patients.21
The mean time required for tracheal intubation in our study was 47.86 ± 11.76 s for ILMA-LW which is close to that observed by Kihara et al., 46 ± 28 s in lightwand-guided tracheal intubation through ILMA.12 However, Dimitriou et al. recorded a lesser time of 31 ± 8 s in light-guided tracheal intubation through ILMA.5 In our study, the mean time required for tracheal intubation through LMA CTrachTM was 64.84 ± 15.97 s. This was significantly longer than that observed with use of ILMA-LW (p < 0.001). Arslan et al. recorded a mean time of 66.3 ± 29.3 s required for tracheal intubation through LMA CTrachTM which is close to our study.23 The time required for tracheal intubation in studies involving LMA CTrachTM varies considerably from 40.8 s to 347.75 s.9,15,17-19,23-25 This wide variation is probably because various investigators have used different study designs and definition of time required for tracheal intubation in their studies.
Ease of intubation was a subjective parameter which was assessed by operator throughout the process of intubation. It was comparable between the two groups. In a study by Yousef et al., median (interquartile range) VAS score for overall subjective intubation difficulty (0, very easy; 100, major difficulty or impossible) with LMA CTrachTM was 12 (1-45).26 In our study, handling of the device was slightly more cumbersome in group ILMA-LW than group CTrachTM due to the dangling lightwand handle. This problem was managed by grip modification as shown in Figure 1. The index finger was used to stabilize the dangling lightwand handle with preloaded ETT. Similar modification was used in LMA CTrachTM group where index finger was used to stabilize the ETT as shown in Figure 2.

Figure 1: Awake intubation using lightwand guided ILMA

Figure 2: Awake intubation using LMA CTrachTM
We observed significantly longer intubation time in LMA CTrachTM group due to excess time required in optimizing view of the glottis on the viewer. Similar results have been obtained by other investigators as well.19,24 Malik et al. observed that the prolongation of tracheal intubation times was not due to the positioning of the LMA CTrachTM, rather it was due to the time required to optimize the view of the glottis.9 Liu et al. also found failure to obtain satisfactory view of larynx despite using multiple maneuvers as a major limitation of LMA CTrachTM.19 We faced difficulty in getting good picture quality and obtaining a satisfactory view in some patients, despite using adjusting maneuvers, focusing using visual test card, antisialagogue preparation and use of antifog solution with LMA CTrachTM. Other authors have also experienced difficulties with LMA CTrachTM such as red-out due to lens touching epiglottis/mucosa or presence of blood, white-out because of secretions or lubricants, black-out due to low light intensity or insufficient depth of insertion.7 Deterioration of light intensity and sharpness of image over the course of applications,7,10 lens getting obstructed by secretions, lubricants and fogging,8,9 deterioration in fiber-optic quality after repeated sterilization9,19 and small visual field, confined within the boundaries of the mask aperture leading to poor views8 have been reported with use of LMA CTrachTM.
There were some limitations in our study. It was impossible to blind the investigator to the device they were using. Application of MILS is subjective; the provider was not blinded and could have been biased towards a technique. It was not a crossover study; the investigator could have performed a particular technique better with fewer complications due to his personal preference. Our study was performed on awake patients and our data may not apply to paralyzed patients.
CONCLUSION
We conclude that performing awake tracheal intubation using lightwand-guided ILMA was significantly faster than LMA CTrachTM with comparable success and ease of intubation, in patients with simulated cervical spine injury after application of manual in-line stabilization.
Conflict of interest: Nil
Authors’ Contribution:
DS & AK – Concept, Conduction of Study work, Manuscript editing
MS – Conduction of Study work, Manuscript editing
REFERENCES
- Meschino A, Devitt JH, Koch JP, Szalai JP, Schwartz ML. The safety of awake tracheal intubation in cervical spine injury. Can J Anaesth 1992;39:114-7. [PubMed]
- Rao GSU. Anaesthetic and intensive care management of traumatic cervical spine injury. Indian J Anaesth 2008;52:13-22. [Free full text]
- Bilgin H, Yyknaz C. Awake intubation through C trach in patients with unstable cervical spine. Anaesthesia 2006;61:513-4. [PubMed] [Free full text]
- Komatsu R, Nagata O, Kamata K, Yamagata K, Sessler DI, Ozaki M. Intubating laryngeal mask airway allows tracheal intubation when the cervical spine is immobilized by a rigid collar. Br J Anaesth 2004;93:655-9. [PubMed] [Free full text]
- Dimitriou V, Voyagis GS. Light-guided tracheal intubation using a prototype illuminated flexible catheter through the intubating laryngeal mask. Eur J Anaesthesiol 1999;16:448-53.
- Tripathi DC, Jha PS, Trivedi LP, Doshi SM, Modia B. LMA CTrach aided endotracheal intubation in simulated cases of cervical spine injury: a series of 30 cases. Saudi J Anaesth 2013;7:165-9. [Free full text]
- Timmermann A, Russo S, Graf BM. Evaluation of the CTrachTM – an intubating LMA with integrated fibreoptic system. Br J Anaesth 2006;96:516-21. [PubMed] [Free full text]
- Lopez AM, Valero R, Pons M, Anglada T. Awake intubation using the LMA-CTrach in patients with difficult airways. Anaesthesia 2009;64:387-91. [PubMed] [Free full text] doi: 10.1111/j.1365-2044.2008.05797.x.
- Malik MA, Subramaniam R, Churasia S, Maharaj CH, Harte BH, Laffey JG. Tracheal intubation in patients with cervical spine immobilization: a comparison of the Airwayscope, LMA C-Trach, and the Macintosh laryngoscopes. Br J Anaesth 2009;102:654-61. [Free full text]
- Hilbert P, Birkmeier M, Stuttmann R. LMA CTrachTM – Results of our first experience with the fiberoptic intubating laryngeal mask airway in 80 patients. South Afr J Anaesth Analg 2006;12:95-9.
- Brain AI, Verghese C, Addy EV, Kapila A, Brimacombe J. The intubating laryngeal mask.II: a preliminary clinical report of a new means of intubating the trachea. Br J Anaesth 1997;79:704-9. [PubMed] [Free full text]
- Kihara S, Watanabe S, Taguchi N, Suga A, Brimacombe JR. A comparison of blind and lightwand-guided tracheal intubation through the intubating laryngeal mask. Anaesthesia. 2000;55:427-31. [PubMed] [Free full text]
- Dimitriou V, Voyagis GS. The intubating laryngeal mask airway (ILMA): disadvantage of being a blind technique. Eur J Anaesthesiol 1999;16:418-9.
- Kihara S, Watanabe S, Taguchi N, Suga A, Brimacombe JR. Tracheal intubation with the Macintosh laryngoscope versus intubating laryngeal mask airway in adults with normal airways. Anaesth Intensive Care 2000;28:281-6. [PubMed] [Free full text]
- Bilgin H, Bozkurt M. Tracheal intubation using the ILMA, C-Trach or McCoy laryngoscope in patients with simulated cervical spine injury. Anaesthesia. 2006 Jul;61(7):685-91. [PubMed] [Free full text]
- Liu EHC, Goy RWL, Chen FG. An evaluation of poor LMA CTrach views with a fibreoptic laryngoscope and the effectiveness of corrective measures. Br J Anaesth 2006;97:878-82. [PubMed] [Free full text]
- Swadia VN, Patel MG. Our preliminary experience with LMA C-Trach. Indian J Anaesth2009;53:312-7. [PubMed] [Free full text]
- Liu EH, Goy RW, Chen FG. The LMA C-TrachTM, a new laryngeal mask airway for endotracheal intubation under vision: evaluation in 100 patients. Br J Anaesth 2006;96:396-400. [PubMed] [Free full text]
- Liu EH, Goy RW, Lim Y, Chen FG. Success of tracheal intubation with intubating laryngeal mask airways: a randomized trial of the LMA Fastrach and LMA CTrach. Anesthesiology 2008;108:621-6. [PubMed] [Free full text] doi: 10.1097/ALN.0b013e318167af61.
- Dhonneur G, Ndoko SK, Yavchitz A, Foucrier A, Fessenmeyer C, Pollian C, et al. Tracheal intubation of morbidly obese patients: LMA CTrachTM vs direct laryngoscopy. Br J Anaesth 2006;97:742-5. [PubMed] [Free full text]
- Dimitriou V, Voyagis GS, Brimacombe JR. Flexible lightwand-guided tracheal intubation with the intubating laryngeal mask Fastrach™ in adults after unpredicted failed laryngoscope-guided tracheal intubation. Anesthesiology 2002;96:296-9. [Free full text]
- Asai T, Shingu K, Latto IP. Use of a lighted stylet for tracheal intubation through the intubating laryngeal mask. Anesth Analg. 1998 Oct;87(4):979. [PubMed]
- Arslan ZI, Yildiz T, Baykara ZN, Solak M, Toker K. Tracheal intubation in patients with rigid collar immobilisation of the cervical spine: a comparison of Airtraq and LMA CTrach devices. Anaesthesia 2009;64:1332-6. [Free full text]
- Arslan ZI, Özdamar D, Yildiz TS, Solak ZM, Toker K. Tracheal intubation in morbidly obese patients: a comparison of the Intubating Laryngeal Mask Airway™ and Laryngeal Mask Airway CTrach™. Anaesthesia 2012;67:261-5. [PubMed] [Free full text] doi: 10.1111/j.1365-2044.2011.06991.x.
- Hoşten T, Gürkan Y, Özdamar D, Tekin M, Solak M, Toker K. Comparison of the Laryngeal Mask Airway (CTrachTM) and direct coupled interface-video laryngoscope for endotracheal Intubation: a prospective, randomized, clinical study. Balkan Med J 2012;29:268-72. [Free full text]
- Yousef GT, Abdalgalil DA, Ibrahim TH. Orotracheal intubation of morbidly obese patients, comparison of Glidescope video laryngoscope and the LMA CTrach™ with direct laryngoscopy. Anesth Essays Res 2012;6:174-9. [PubMed] [Free full text] doi: 10.4103/0259-1162.108304.
