
Faisal Shamim, FCPS1, Muhammad Yahya, MBBS2, Mubasher Ikram, FCPS3
1Associate Professor; 2Resident
Department of Anesthesiology, Aga Khan University Hospital, Stadium Road, Karachi, (Pakistan)
3Associate Professor & Section Head, Otolaryngology, Department of Surgery, Aga Khan University Hospital, Stadium Road, Karachi, (Pakistan)
Correspondence: Dr Faisal Shamim, Department of Anesthesiology, Aga Khan University, Stadium Road, Karachi – 74800 (Pakistan); Phine: +923332229440, +922134934294; E-mail: faisal.shamim@aku.edu
ABSTRACT
Thyroid enlargement or goiter has been considered a risk factor for difficulty in airway management during anesthesia and surgery. Moderate to huge size along with retro-sternal extension makes it an anticipated difficult airway scenario. In this report, we present a case of huge goiter with compression symptoms and patient cannot be intubated by conventional direct laryngoscopy at a district hospital a week ago. CT scan revealed extension of mass into superior mediastinum compressing right brachiocephalic vein and superior vena cava. We successfully performed awake fiberoptic intubation with local/topical anesthesia of airway. We have discussed the significance of careful approach, planning and preparation in the management of such a case.
Key words: Goiter; Difficult airway; Awake fiberoptic intubation
Citation: Shamim F, Yahya M, Ikram M. Awake fiberoptic intubation in a patient with known difficult airway due to huge thyroid goiter. Anaesth, Pain & Intensive Care 2017;21(1):94-97
Received: 18 Dec 2016; Reviewed: 26 Jan 2017; Corrected: 27 Feb 2017; Accepted: 10 Mar 2017
INTRODUCTION
Over 1.9 billion people across the world are at risk of developing thyroid enlargement termed ‘goiter’.1 Prevalence of giant goiter in Pakistan is reported to be 26.08% in patients undergoing thyroid surgery.2 Enlarged goiter with compromised airway is an ineradicable risk of difficult airway and hence can lead to airway crisis. Risk of difficult intubation in thyroid surgery is reported to be 11.1%3 hence awake fiberoptic intubation (AFOI) is a successful and safe choice.4
Here, we present a case of successful airway management with awake fiberoptic intubation in total thyroidectomy for huge goiter. The patient was referred from a district hospital in a distant city to our tertiary care center because of failed conventional direct laryngoscopy and intubation and non-availability of advanced airway equipment and skills.
CASE HISTORY
Sixty-five years old, 59 kg woman presented with a large multinodular goiter to otorhinolaryngology (ENT) clinic. She had this problem for last 10 years with progressive enlargement and history of palpitation. Since last one month, goiter hugely increased with subsequent development of shortness of breath, dysphagia and hoarseness. She was admitted for total thyroidectomy 1 week back in a peripheral hospital of neighbouring province but surgery was deferred, as patient couldn’t be intubated despite multiple attempts.
In preopeartive assessment and examination, patient was conscious, co-operative. The neck swelling was 20.5 x 14.9 x 11.7cm in size extending from lower jaw to sternal notch (Figure 1). The lower limit of the swelling was neither visualized nor palpable. In airway examination, mouth opening was < 2 fingers due to large thyroid mass interfering with mouth opening. Malampatti was grade IV; incisors were protruding, limited neck extension, and severely restricted neck flexion.

Figure 1: Goiter extending from lower jaw to sternal notch
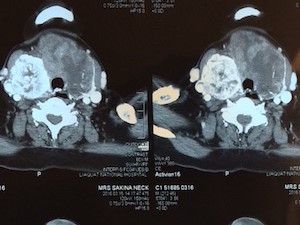
Figure 2-A: CT scan neck and chest
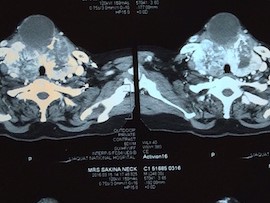
Figure 2-B: CT scan neck and chest
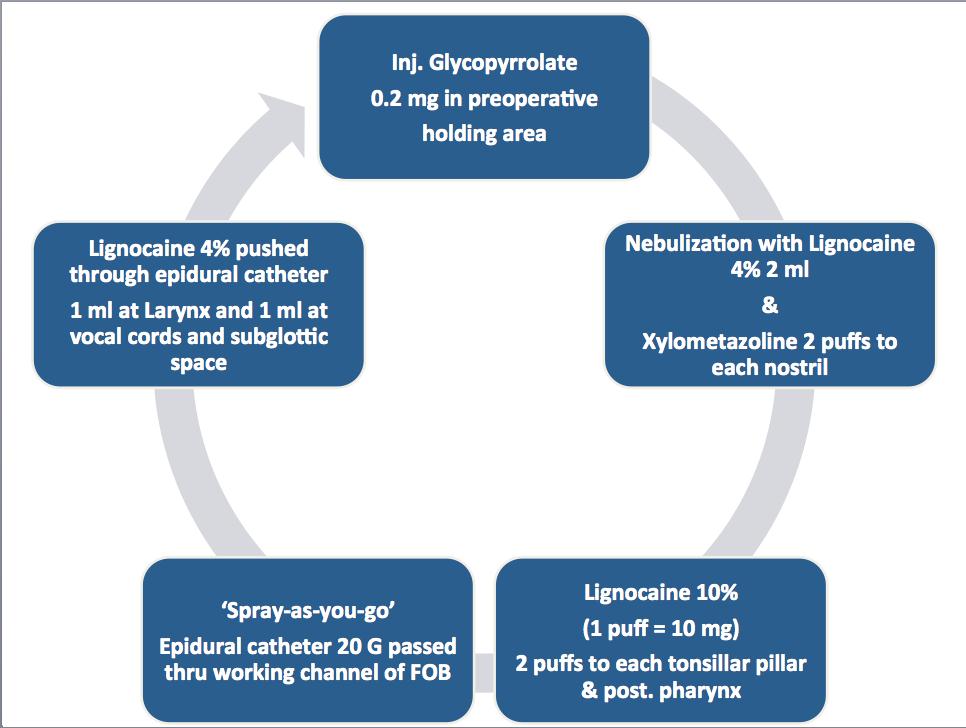
Figure 3: Outlining preparation of topical anesthesia for airway
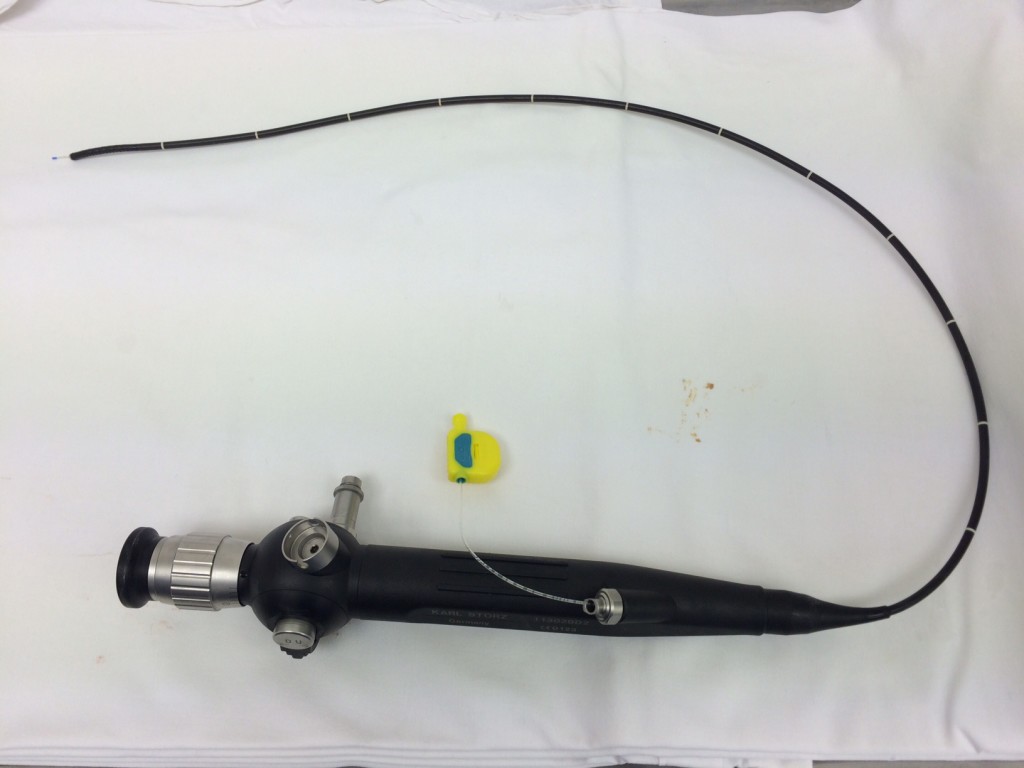
Figure 4: Tip of the epidural catheter protruding at distal end of fiberoptic bronchoscope for spray-as-you-go technique
Indirect laryngoscopy performed by ENT surgeon revealed immobile right-sided vocal cord. The findings of CT scan neck and chest (Figure 2-A & B) were multiple masses in multinodular goiter with areas of necrosis and fibrosis in both thyroid lobes and isthmus. Largest one was seen in Left lobe measuring 9.5 cm × 4.9 cm × 7.9 cm. The mass on right side was seen extending into the superior mediastinum, which was abutting and compressing right brachiocephalic vein and superior vena cava. The goiter was compressing trachea medially and sternocleidomastoid muscle anteriorly. Laterally these masses were abutting carotid vessels bilaterally and superiorly thyroid cartilage.
So the history of failed intubation just a week back, anticipated difficult mask ventilation and tracheal compression after induction of general anesthesia fiber optic intubation under topical / regional anesthesia of airway in a conscious state was planned. Safe dose of lignocaine (5 mg/kg) was calculated. Difficult airway management trolley with rigid bronchoscope and jet ventilation was kept ready. Cardiothoracic surgeon was consulted and requests his availability in operating room for possible hemodynamic collapse. The patient was made aware of the steps involved and written consent was taken. No preoperative sedative / anxiolytic medication was given due to risk of airway obstruction.
The preparation of topical anesthesia for airway is outlined in Figure 3. In preoperative holding area, inj. glycopyrrolate 0.2 mg intravenous was given to dry airway mucosa. Then, she was nebulized with 4% lignocaine 2 ml. Xynosine 2 puffs sprayed to each nostril. In operating room standard monitors (ECG, pulse oximeter, and NIBP) were attached, and the baseline vitals were recorded. Invasive arterial line was placed in left radial artery. The operating table was kept in head-up (30°) position. 2 puffs Lignocaine 10% (1 puff = 10mg) were sprayed on both tonsillar pillars and posterior pharynx. Reinforced endotracheal tube (ETT) 6.5 mm was loaded on fiberoptic bronchoscope (FOB), which was attached with camera monitor. An epidural catheter 20 G was passed thru injection port of fiberscope for ‘spray-as-you-go’ technique (Figure 4). Nasal airway was gently passed through left nostril and connected with anesthetic circuit for 100% oxygen. The FOB was introduced through right nostril and advanced towards nasopharynx, then oropharynx until epiglottis was seen. Slowly progressed into laryngeal opening and here 1 ml 4% lignocaine pushed through epidural catheter. The vocal cords (VC) are visualized and fiberscope further advanced to pass through VC where again 1 ml lignocaine 4% was sprayed over the vocal cords and subglottic space. The FOB was positioned just above the carina and ETT was railroaded over the fiberscope. The ETT placement was reconfirmed with capnography and then secured. Anesthetic induction was done with inj. propofol 50 mg, fentanyl 150 µg and atracurium 40 mg.
Total thyroidectomy along with retrosternal extraction of goiter was done successfully. The patient remained hemodynamically stable throughout the procedure. Due to high probability of tracheomalacia associated with long standing history and immobile right vocal cord preoperatively, tracheostomy was done before awakening the patient from anesthesia. She remained stable in postoperative period and hence discharged from the hospital on 5th day.
DISCUSSION
In some parts of the world, thyroid diseases are common due to deficiency of iodine with an incidence of 10–15% in adult populations.1 As prevalence of huge goiter is quite significant in our region2, there is a serious need to develop a strategy in order to manage patients with huge goiter considering potential airway problems and available options. Anesthetic management of a patient with goiter depends on the size of the goiter, vascularity, compression on the surrounding organs and sub-sternal extension.
WHO has classified goiter according to the size, according to which Class 0-palpable mass within neck structure and Class I-visible, palpable and undermines the curves and the neckline. Class II is a very large goiter with retrosternal extension that leads to tracheal deviation, compression of trachea and esophagus.5 Our patient was class II type. We anticipated difficult airway management in our patient because of multiple factors including reduced mouth opening (inter-incisor distance 1.5 cm), protruding teeth, compression and deviation of trachea from the midline, upper airway obstruction as evident from the pressure symptoms and failed conventional laryngoscopy and intubation.
There are multiple modalities to manage the difficult airway in the patient with thyroid enlargement. Awake tracheostomy under local anesthesia with huge goiter and poor anatomic landmarks is questionable6 Lifting of the thyroid mass or rigid bronchoscopy can only help keep the airway patent. Direct laryngoscopy has no role in this situation. Keeping the clinical symptoms in mind and imaging studies, our patient was in need of an awake fiberoptic intubation. This can prevent conditions like “can’t ventilate and can’t intubate” scenarios occurring after induction of anesthesia due to a complete tracheal collapse.
Several authors have reported that fiberoptic intubation (FOI) can be achieved with considerable hemodynamic stability under local anesthetic when combined with sedation while producing minimal patient discomfort7. Topical anesthesia to the nasal and/or oral mucosa in combination with a method to anesthetize the laryngeal/tracheal structures is the most effective and the most commonly chosen plan.8 Srivastava et al reported a case of 58 years old female with huge goiter, which was successfully intubated with fiberoptic bronchoscope using loco-sedative technique.4 Midazolam and fentanyl was were used for sedation along with 5L oxygen. Topical anesthesia was achieved with 2% lignocaine jelly in nostrils, gargles of 2% lignocaine aqueous solution and 4mls of 4% lignocaine nebulization. Lignocaine was also given through drug port of the bronchoscope. We completely avoided sedation to prevent any further airway compromise. One must caution about liberal use of local anesthetics that is also associated with sudden airway collapse during awake fiber optic intubation.9, 10
In conclusion, there is no single best modality for difficult airway management but when it comes to a known failed airway and obvious factors like thyroid enlargement, awake intubation with fiberoptic bronchoscope will be the most suitable choice. Decision should be made after a thorough discussion with the surgeon and the patient.
Acknowledgement: The authors would like to thanks all team members of operating room 7 (ENT / Head & Neck) for their efforts and clinical support
Conflict of Interest: None declared
Author contribution: This is to certify that the manuscript has been read and approved by all the authors, the requirements for authorship have been met, and each author believes that the manuscript represents honest work.
REFERENCES
- Lazarus JH, Delange F. Prevalence of iodine deficiency worldwide. The Lancet. 2004;363:901. [PubMed]
- Ahmed I, Awan ZI, Khan SA, Rasul S, Ishtiaq S. Giant goiter: not common in endemic areas of Pakistan. A 10 years experience. Progressive.4:5.
- Amathieu R, Smail N, Catineau J, Poloujadoff MP, Samii K, Adnet F. Difficult intubation in thyroid surgery: myth or reality? Anesth Analg. 2006;103:965-8. [PubMed]
- Srivastava D, Dhiraaj S. Airway management of a difficult airway due to prolonged enlarged goiter using loco-sedative technique. Saudi J Anaesth. 2013;7:86. Saudi J Anaesth. 2013 Jan;7(1):86-9. doi: 10.4103/1658-354X.109829. [PubMed] [Free full text]
- Bartolek D, Frick A. Huge multinodular goiter with mid trachea obstruction: Indication for fiberoptic intubation. Acta Clin Croat. 2012;51:493–8. [PubMed]
- Chakera A, Van Heerden PV, Van Der Schaaf A. Elective awake intubation in a patient with massive multinodular goiter presenting for radioiodine treatment. Anaesthesia and intensive care. 2002;30:236-9. [PubMed] [Free full text]
- Khetarpal R, Chatrath V, Dhawan A, Attri JP. Regional anesthesia in difficult airway: The quest for a solution continues. Anesth Essays Res. 2016 May-Aug;10(2):178-83. doi: 10.4103/0259-1162.167829.[PubMed] [Free full text]
- Ovassapian A. Fiberoptic Endoscopy and the Difficult Airway. 2nd ed. Philadelphia: Lippincott-Raven Press, 1996.
- Woodall NM, Harwood RJ, Barker GL. Complications of awake fibreoptic intubation without sedation in 200 healthy anaesthetists attending a training course. Br J Anaesth. 2008 Jun;100(6):850-5. doi: 10.1093/bja/aen076. [PubMed]
- Collins SR, Blank RS. Fiberoptic Intubation: An Overview and Update. Respir Care. 2014 Jun;59(6):865-78; discussion 878-80. doi: 10.4187/respcare.03012.
