
Kale Sunti, MD*, Aggarwal Shipra, MD**, Talwar Vandana, M.D***, Sengar Piyush, MD***
*Senior Resident, **Assistant Professor, ***Professor
Department of Anesthesiology, Intensive Care and Pain Medicine, Safdarjung Hospital, New Delhi, (India)
Correspondence: Dr. Shipra Aggarwal, Department of Anesthesiology, Intensive Care and Pain Medicine, Safdarjung Hospital, New Delhi-29 (India); Phone: 09811420886; E-mail: shipra.mamc@gmail.com
Key words:Fiberoptic endoscopic sinus surgery; ECHO; Apical hypertrophic cardiomyopathy
Citation: Sunti K, Shipra A, Vandana T, Piyush S. Apical hypertrophic obstructive cardiomyopathy: a rare entity. Anaesth Pain & Intensive Care 2014;18(2):217-218
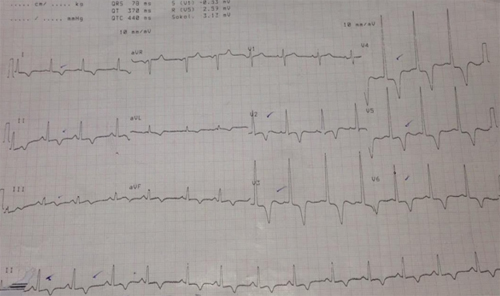
A sixty years old male weighing 80 kg presented to us for FESS (fiberoptic endoscopic sinus surgery). Patient was clinically asymptomatic for any cardiac illness with good effort tolerance. Pre-operative ECG showed global deep T-wave inversion in lead II & lead V of the ECG [Figure 1] for which a cardiology referral was sought. The ECHO report was normal as per the cardiologist and no further cardiology intervention was advised.
Figure 1: ECG trace of the same patient
The baseline blood pressure and heart rate were 150/90 mmHg and 77/min respectively. Anesthesia was induced with intravenous midazolam 2 mg, fentanyl 100 µg and propofol 100 mg. Vecuronium bromide 8 mg was given to facilitate endotracheal intubation. Soon after induction, the blood pressure dropped to 67/44 mmHg and HR dropped to 49/ min. The BP and HR remained 86/58 mmHg and 54/ min even after treatment with atropine and mephentermine. The procedure was abandoned in view of further hemodynamic perturbations. Proseal LMA No.4 was inserted till the effect of muscle relaxant wore off. A review cardiology opinion was considered.
Careful cardiology re-evaluation revealed apical wall thickness on echocardiography with normal ejection fraction of 60 %. Angiography report was normal. A provisional diagnosis of apical hypertrophic cardiomyopathy (AHCM) was made and confirmed by cardiac MRI. Detailed family history revealed familial penetrance. AHCM is a milder form of obstructive HCM which involves the apex of left ventricle.1,2 Prevalence is 15% in Japanese population and ≤3 % elsewhere. AHCM is frequently sporadic but may have an autosomal dominant inheritance. The mean age of presentation is 41.4 ±14.5 years with male predominance. Generally asymptomatic (54%), it may mimic acute coronary syndromes with morbid events including sudden cardiac arrest[3].
The most frequent ECG findings are negative T waves (≥ depth 10 mm ) in pre cordial leads (93 %) and left ventricular hypertrophy ( 63 %).1 The diagnostic criteria for AHCM include left ventricular hypertrophy with apical wall thickness > 15 mm and a ratio of maximal apical to posterior wall thickness > 1.5 mm on echocardiography. There is characteristic “ace of spades” pattern on ventriculogram. Cardiac MRI is considered to be the most sensitive diagnostic tool. Treatment includes beta blockers, calcium channel blockers and alcohol ablation.4
Anaesthetic challenges in cases of AHCM are related to rarity of condition in non- Japanese population and ECG findings mimicking acute coronary syndromes. Also, the condition can be easily missed on ECHO.2 Asymptomatic patients presenting with typical ECG findings of global deep T wave inversion should arouse a high degree of clinical suspicion of AHCM. The general principles of anesthesia include minimising sympathetic stimulation, maintenance of adequate preload and afterload, avoidance of tachycardia and increased cardiac contractility.4,5 There is a paucity of literature on anaesthetic management in cases with AHCM. Though prognosis is better than obstructive HCM, a careful and complete cardiac evaluation will help in reducing peri-operative complications associated with anesthesia and surgery. In our case after establishing the diagnosis and discussing the risk involved with general anesthesia, it was decided to perform the procedureunder local anesthesia with monitored anesthesia care.
REFERENCES
- Yusuf SW, Bathina JD, Banchs J, Mouhayar EN, et al. World J Cardiol 2011;26(3):256-59.
- [PubMed][Free Full Text]
- Ates M, Kwong RY, Lipton MJ, TatliS. Apical hypertrophic cardiomyopathy. Tex Heart Inst J. 2006; 33:408-09. [PubMed][Free Full Text]
- Ridjab D, Koch M, Zabel M, Schultheiss HP, et al. Cardiac arrest and ventricular tachycardia in Japanese type apical hypertrophic cardiomyopathy. Cardiology 2007;107:81-86. [PubMed]
- Chan SM, Wu CT, Wong CS, Cherng CH, Lu CH. Apical hypertrophic cardiomyopathy mimicking coronary artery disease with unstable angina. J Med Sci 2008;28:035-038.
- Autore C, Brauneis S, Apponi F, Commisso C , Pinto G, Fedele F. Epidural anesthesia for cesarean section in patients with hypertrophic cardiomyopathy: a report of three cases. Anesthesiology 1999;90:1206-07. [PubMed][Free Full Text]
