
Rabia Sajjad, FCPS*, Ch. Amjad Ali, MCPS, FCPS**, Muhammad Zia-ul-Haq, MCPS, FCPS***,
Amjad Iqbal, MCPS, FCPS****
*Consultant obstetrician & gynecologist; **Consultant anesthesiologist; ***Consultant pediatrician; ****Consultant anesthesiologist & HoD
Combined Military Hospital, Rawalpindi (Pakistan)
Correspondence: Dr. Rabia Sajjad, Consultant obstetrician & gynecologist, Combined Military Hospital, Sargodha. (Pakistan); Phone: +92 321 4359488; E-mail: rabia999@ymail.com
ABSTRACT
Objective: To analyze the rate, the frequency of different indications and the most common indication of cesarean sections in Military Hospital Rawalpindi.
Study Design: Cross sectional study
Place and Duration: Obstetrics and Gynecology Department of Military Hospital Rawalpindi from September 2011 toFebruary 2012.
Methodology: A total of 3555 pregnant females delivered during study period were enrolled in the study. Health volunteers and the cases of uterine rupture, pregnancy with fetal anomaly, or termination of pregnancy were excluded from the study. All patients were admitted in labor room. Detailed obstetric and gynecological history was taken. Detailed general physical examination and obstetric examination was done. Baseline investigations were checked. Fetal anomalies were ruled out by anomaly scan. Strict fetomaternal monitoring was done during labor. Cervical foley catheter and prostaglandin E2 (Prostin®) tablets were used for induction according to Bishop score. Clinical record of all patients, including mode of delivery and indication, was analyzed in terms of percentage and frequency and documented in a special performa after written informed consent. Filled performas were attached with patient’s case notes.
Results: Patients enrolled in the study over six months were 3555, out of which 1620 (45.5%) were delivered by cesarean section, 1901 (53.4%) were spontaneous vaginal deliveries and 34 (0.9%) were delivered by vaginal birth after cesarean (VBAC). The rate of cesarean section in our study was 45.5% and the most common factor was repeat cesarean section (44.4%), followed by failed trial of labor (27.1%) and fetal distress seen in 165 (10.1%) cases.
Conclusion: The rate of cesarean section in our study was 45.5% and the most common factor was repeat cesarean section 44.4%.
Key words: Cesarean section; PPH; Pfannenstiel incision; Audit; Primigravida.
Citation: Sajjad R, Ali CA, Iqbal A, Sajjad N, Haq MZ. An audit of cesarean sections in Military Hospital Rawalpindi. Anaesth Pain & Intensive Care 2014;18(2):172-75
INTRODUCTION
Major obstetric procedure with marked increase in rate is nothing else but cesarean section (CS),1 which has a rising rate not only in our country but all over world.1
CS is rapid method of delivery by abdominal route but associated with maternal and fetal complication. Infection, hemorrhage, complication of anesthesia bladder damage, prolonged hospital stay and delayed recovery are common complications when compared with vaginal delivery, which is natural way of delivery associated with rapid recovery and less hospital stay. Postpartum hemorrhage (PPH), especially primary PPH is one of the top five causes of maternal mortality in both developed and developing countries.2
Although due to modified and advanced surgical techniques, CS has become safer, but it is still not as safe as normal vaginal delivery.3
Countries with a lowest perinatal mortality have lowest CS rate, just around 10%.4 Morbidity with CS is 5-10 times higher than that of normal delivery..5 Common factors of CS in our population are repeat cesarean section, fetal distress and cephalopelvic disproportion (CPD).6,7
The objective of this study was to find the prevalent rate of cesarean sections, the factors responsible and the most common indication for CS in our institution and to put forth recommendations to contain the high rate.
METHODOLOGY
This cross sectional study was done in Obstetric & Gynecology Department of Military Hospital Rawalpindi from September 2011 to February 2012.
All women delivered in this period, irrespective of parity, were included in the study from outpatient department. Health volunteers, cases of uterine rupture and pregnancy with fetal anomalies for termination were excluded from the study. Patients were admitted and informed consent was taken. History regarding patient’s age, marital status, obstetric and gynecological background was noted. Patients were investigated about gestational age, fetal movement, vaginal bleeding and any history of dai handling. Documents were reviewed for indications of previous cesarean sections if any. Women were examined for pallor, blood pressure, pulse rate, lymph nodes, thyroid and body mass index. Detailed obstetrical examination for fundal height, fetal heart rate, lie, presentation and engagement of presenting part was done. Scar tenderness was also checked. Bishop score was calculated and adequacy of pelvis was checked especially in patients with previous cesarean with CPD. Base line investigation including blood group and Rhesus factor, complete blood count and urine examination, hepatitis B and C screening and blood glucose level were done. Ultrasound was done for fetal growth and to detect any congenital anomalies.
Consent for induction was taken. Cervical foley and tab. prostaglandin E2 [Prostin E2 (by Pfizer Inc.)] was used for induction according to bishop score. Strict fetal monitoring (intrapartum CTG, intermittent auscultation of fetal heart) with Pinnard fetoscope was done after every 15 min during first stage of labor and after every contraction in second stage of labor. Artificial rupture of membrane was done at 4 cm and color of liquor was noted. Fetomaternal monitoring was continuously done in labor. Clinical record of all patients including mode of delivery and indication was analyzed in terms of percentage and frequency and documented on a performa. Completed performas were attached with patient’s case notes.
Data analysis: Descriptive statistics were used to describe the data. Tables and graphs were used to depict the results.
RESULTS
In our study, a total of 3555 deliveries were conducted over a period of six months. Out of this, the number of parturients delivered by CS was 1620 (45.5%) and 1901(53.4%) were delivered by SVD. Elective CS was done in 786 (48.5%) patient and 834 patients underwent emergency CS (51.48%) (Figure 1). All cesarean sections were done by Pfannenstiel incision under spinal anesthesia.
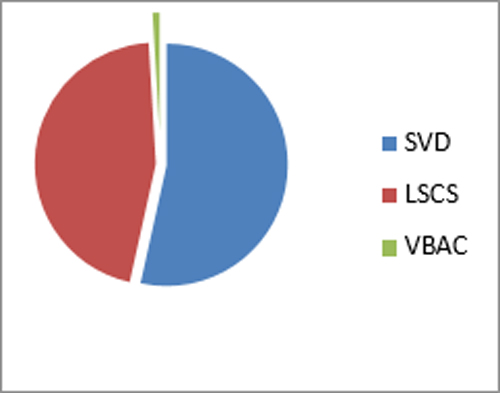
Figure 1: Different modes of deliveries
Out of 3555 parturients, 1932 (54.35 %) were booked ones, while the rest of them were unbooked and received as emergency cases.
Regarding parity, 828 (23.2%) women were primigarvida, 2213 (62.2%) were multigravida and 514 (14.4%) were grandmultipara (Table 1).
Table 1: Parity of the patients (n=3355)
|
Parity |
Frequency (n) |
% |
| Primigravida |
828 |
23.3 |
| Multipara |
2213 |
62.3 |
| Grand multipara |
514 |
14.4 |
| Total |
3355 |
100 |
Total rate of CS was 45.5% over six month of period and repeat cesarean was common indication seen in 720 (44.4%) cases (Table 2). Antepartum hemorrhage was seen in 50 (3%) of cases; 114 (7%) of patients were operated for CPD, 65 (4%) for malpresentation and 35 (2.09%) due to eclampsia. Failed trial of labor was the second most common indication seen in 440 patients, while fetal distress was an indication in 165(10.1%) of the parturients (Table – 2).
Table 2: Indications of C-section (n=1620)
|
Indications |
Frequency (n) |
% |
| Repeat C-section |
720 |
44.4 |
| APH* |
50 |
3 |
| CPD** |
114 |
7 |
| Failed progress |
440 |
27.1 |
| Fetal distress |
165 |
10.1 |
| Malpresentation |
65 |
4 |
| Eclampsia |
34 |
2.09 |
| Others |
32 |
1.9 |
*Antepartum hemorrhage
**Cephalopelvic disproportion
No anesthesia related mortality was seen in our patients. There was no perinatal maternal morbidity and mortality. All patients were discharged on 2nd or 3rd post op day.
DISCUSSION
CS is the major obstetric operation, the ratio of which has dramatically increased all over the world.1 The mostimportant determinant of future obstetric course of any woman happens to be primary CS which should be avoided.8 In our hospital the rate of CS was high probably because majority of the pregnant women had been booked with traditional birth attendants (dai’s), lady health visitors or GP’s, and majority of them were referred to our tertiary care hospital due to anticipated difficulties in SVD. Lack of awareness or simply neglect on the part of parturients was another contributing factor to the high rate. During 1985, CS rates in the United States and in the United Kingdom were 18-23%.9 It was still at 21% in 1996 and rose to 31.3% from 2009 to 2012.10
The rate has risen to 46% in China – the world’s highest rate. Pregnant woman’s reluctant attitude towards natural birth is regarded as important factors behind China’s high cesarean sections rate.11 Rate lies at 25% and above in many Asian, European and Latin American countries. In Italy the Caesarean section rate is 40%, while in the Nordic countries it is 14%.11 In our country, a study put the rate to be 35% in 2009 in a teaching hospital,12as compared to 45.5% over a period of six month in the current study. The difference in the two rates raises many questions, which need to be addressed.
The commonest indication in our study was repeat CS (44.4%)(Table 2). A researcher put it at 31.2% in another study,10,13 while a similar observation was made by Yudkin,14 so it was concluded that first CS should be avoided as far as possible.
A total of 23.2% (828) patients were primigravida in our study (Table 1).A study in Taiwan proved significant relationship between maternal age and increasing rate of CS.15 The elderly primigravida is defined as a woman who conceives first time at the age of 35 years or more. Due to changed life styles for higher education and career advancement, childbearing is postponed, resulting in an increase in maternal age.16 This retrospective study was done during 2003 to 2008 comparing the pregnancy outcome in elderly primigravidae with younger primigravidae aged 20-25 years. Outcome was in terms of mode of delivery. Regarding complications, anemia, ante-partum hemorrhage, malpresentation, diabetes mellitus, intra-uterine growth restriction (IUGR) were statistically higher in the elderly primigravidae than in the younger group (p<0.05).16
Pfannenstiel incision is associated with fewer complications. In our study all CS were done by Pfannenstiel incision and no CS was done by midline incision. Pfannenstiel incision and transverse muscle-cutting Maylard incision show no differences in intraoperative characteristics, postoperative morbidity or pain.17
In our study 45.6% parturients were unbooked as compared to an earlier study conducted at Liaquat University Hospital Hyderabad, where 75.3% were unbooked. Reason may probably be a lack of education, access to the healthcare facilities and a lack of awareness in that area.12
In our study, no anesthesia related complication was seen but in another study difficult intubation was seen in 0.5% of the patients.12
In our study, patients with previous CS were more prone to have subsequent CS (Table 2). A study conducted to assess the trend of CS and to identify patient groups with an increased risk for CS, compared CS in year 2000 (N=10540) with year 2008 (N=1401). The authors concluded that over a period of eight years, the CS rise is most prominent in women with previous sections with fall in rate of induction.18 A research done in 2003 to assess the influence of increased use of health-care services on rising rates of CS in China concluded that the increase in the use of antenatal care, especially ultrasound scanning, was associated with an increase in caesarean rate.19
In most of the countries, around one third of CS are performed electively and two third are performed as emergency procedures. Primary CS has major contribution in determining the future obstetric course of a woman.20
An audit for reducing rate of primary CS was done with objective to evaluate how the implementation of universally acceptable standards may affect rates for primary CS, without compromising maternal or fetal health. New guidelines were implemented after the first audit. The rates of CS, induction of labor, failed induction, and maternal and fetal outcomes were compared before and after the implementation of the guidelines.20 Primary emergency CS rate decreased from 16% to 12% with increase in rate of induction rate showing reduction in CS rate by implementation of standard guidelines.20 Another audit over two years was done to determine role of standard measurements for improvement in rate of CS. CS rate decreased from 20·9% to 19·2%. The emergency section rate was unchanged at 14·8% in 1998 (70·9% of total) and 13·6% in 1999 (70·8% of total). Main reasons for emergency sections were either failure to progress (59% in 1998, 47% in 1999) or fetal distress (27% in 1998, 34% in 1999).21
Mode of delivery has great impact on women’s life so this important decision should be made at consultant level to get good maternal, fetal outcome and to give women their best obstetrical future.
Recommendations: On the basis of the results of our study, we offer following recommendations to concerned authorities;
- Peer discussion on the necessity of CS is required.
- Accurate documentation of indication for CS is recommended.
- Repeat CS should be avoided if possible.
- How to avoid CS in primigravidae is an area worth consideration for extensive research.
- Patients should be counseled for VBAC in the hospital.
- Induction at a poor Bishop score should be strongly discouraged.
- Diagnostic procedures during the labor stage, e.g. fetal blood sampling and cardiotocography, are essential.18
- Particular attention is required on CS in relation to preterm delivery and breech presentation.18
- External cephalic version should be offered to uncomplicated breach at 37 weeks of gestation.
- Decision of CS should be taken by senior consultant. It will definitely reduce its rate.
CONCLUSION
Rate of cesarean section in our institution was found to be high (45.5%) as compared to earlier studies at home as well as in the other countries; the most common factor observed in our study was repeat cesarean section. A national level consensus guideline is required to control the rising rate of cesarean section, especially in the primipara.
REFERENCES
- Lee SI, Khang YH, Lee MS. Women’s attitude towards mode of delivery in South Korea: a society with high cesarean section rates. Birth 2004;31:108-16. [PubMed]
- Mousa HA, Treatment of primary post partum haemorrhage. Cochrane Database Syst Rev. 2014;2:CD003249. [PubMed]
- Sachs BP, Koblein C, Castro MA. The risks of lowering the cesarean -delivery rate. N Eng J Med 1999;340:54-7. [PubMed][Free Full Text]
- Sweet RD, Ledger WJ. Puerperal infectious morbidity. Am J Obstet Gynaecol 1973;117:1093-100. [PubMed]
- World Health Organization: Appropriate technology for birth. Lancet 1985;326(8452):436-37. [PubMed]
- Gonen R, Tamir A, Ohel G. Variable associated with successful vaginal birth after one cesarean section score. Am J Pernatol 2004;21:447 -53. [PubMed]
- Quddusi H, Anwar S. Trial of labor after cesarean delivery: a study of 100 cases. Pak J Med Res 2005;44:54-6.
- Yudkin PL, Redman CWG. Cesarean section dissected, 1978 -1983. Brit J Obstet Gynecol1986;93:135-44. [PubMed]
- Notozoan FC, PlackPJ, Taffel SM. Comparison of national cesarean section rates. N Engl J Med1987;316:386. [PubMed][Free Full Text]
- “C-section rates around globe at ‘epidemic’ levels. Avaialable at http://www.nbcnews.com/id/34826186/#.UxldVD-Sz7Q 12 January 2010. Accessed on March 2013 [Access Online]
- Safe Prevention of the Primary Cesarean Delivery. American College of Obstetricians and Gynecologists (the College) and the Society for Maternal-Fetal Medicine. March 2014. Available at https://www.acog.org/Resources_And_Publications/Obstetric_Care_Consensus_Series/Safe_Prevention_of_the_Primary_Cesarean_Delivery. Accessed on March 2013. [Access Online]
- Khawaja NP1, Yousaf T, Tayyeb R. Analysis of caesarean delivery at a tertiary care hospital in Pakistan. J Obstet Gynaecol. 2004;24:139-41. [PubMed]
- Hou Lei. C-section rates highest in China, reasons mixed. China Daily. [Access Online]
- Notzon FC, Cnattingius S, Bergsjo P, Cole S, Taffel S, Irgens L, et al. Cesarean section delivery in 1980’s: International comparison by indication. Am J Obstel Gynaecol1994;170:495 -504. [PubMed]
- Kozinszky Z, Orvos h, zoboki T, Katona M, Wayda K, Pál A, Kovács L. Risk factors for cesarean section of primiparous women aged over 35 years. Acta Obstet Gynecol Scand 2002;81:313-6. [PubMed]
- Eke AC, Eleje GU. The pregnancy outcome in elderly primigravida five year review (Dissertation); Department of Obstetrics and Gynecology, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria
- Giacalone PL, Herisson C, Hedon B, Laffargue F. Pfannenstiel versus Maylard incision for cesarean delivery: A randomized controlled trial. Obstet Gynecol 2002;99:745-50. [PubMed]
- Delbaere I, Cammu H, Martens E, Tency I, Martens G, Temmerman M. Limiting the caesarean section rate in low risk pregnancies is key to lowering the trend of increased abdominal deliveries: an observational study.BMC Pregnancy Childbirth 2012;12:3. [PubMed] [Free Full Text]
- Guo Sufang, Sabu S Padmadas, James J Brown, R William Stones. Delivery settings and caesarean section rates in China. Bulletin of the World Health Organization 2007;85:755–62. [Free Full Text]
- Sheikh L, Tehseen S, Gowani SA, Bhurgri H, Rizvi JH, Kagazwala S. Reducing the rate of Primary Caesarean Sections – an Audit. J Pak Med Assoc 2008;58:444-8. [PubMed]
- Bruce D, Stone S, Harding K. Evaluation of emergency caesarean sections–completion of the audit cycle in a Central London teaching hospital. J Obstet Gynaecol 2002;22:273-278. [PubMed]
