
Alka Chandra, MD, DNB, MBA (Hospital Management)1, Anshumali Gupta,DNB2, Divya Arora, DA3, Sanjeev Singh Chauhan, MD, DM, DNB4
1Senior Specialist; 2Assistant Professor, 3Resident,
Department Of Anaesthesia & Critical Care, North Delhi Municipal Corporation (NDMC) Medical College & Hindu Rao Hospital, DR. J.S. Kkaranwal Memorial Road, Malka Ganj, New Delhi, Delhi 110007, (India)
4Neurologist, Department of Neurology, North Delhi Municipal Corporation (NDMC) Medical College & Hindu Rao Hospital, DR. J.S. Kkaranwal Memorial Road, Malka Ganj, New Delhi, Delhi 110007, (India)
Correspondence: Dr Alka Chandra, 802, South Delhi Apt, Sector 4, Dwarka, New Delhi (India); Phone: +9560044454; E-mail: dralkadelhi@yahoo.co.in
ABSTRACT
A 30 year old postpartum female presented to us with clinical features of headache, vomiting, hypertension, blurring of vision and altered sensorium. On investigating she had anemia and deranged kidney function tests. The computerised tomography (CT) scan head findings were suggestive of posterior reversible encephalopathy syndrome (PRES), which was confirmed by magnetic resonance imaging (MRI) of the brain. The patient responded to symptomatic treatment and was discharged with normal MRI of head and normal kidney function test. We would like to highlight this neuro-radiological condition, which if treated promptly, has a good outcome.
Key words: Hypertension; Kidney function tests; Posterior reversible encephalopathy syndrome; PRES
Citation: Chandra A, Gupta A, Arora D, Chauhan SS. Acute kidney injury and posterior reversible encephalopathy syndrome- a case report. Anaesth Pain & Intensive Care 2017;21(3)377-379
Received – 20 Aug 2017; Reviewed – 10 Sep 2017; Corrected & Accepted – 15 Sep 2017
INTRODUCTION
Posterior reversible encephalopathy syndrome (PRES) is characterized by symmetrical bilateral sub cortical-cortical hyper intensities in T2 weighted images. The parieto-occipital lobes are more often involved. The regional heterogeneity of the arterial sympathetic innervation which is maximal in the anterior circulation is the reason for occipital lobes and other posterior brain regions to be at higher risk for hydrostatic edema.1
It is a clinical and neuro-radiological entity characterized by a disorder of cerebrovascular autoregulation whose neuro-radiological and clinical alterations are usually completely reversible.2 Although an ischemic evolution is possible , prompt treatment is necessary to prevent irreversible brain damage.3 Inspite of being increasingly recognized neurological disorder, its pathogenesis remains poorly understood. Through this case report we have tried to discuss the details of available diagnostic and management tools.
CASE REPORT
A 30 years old woman, with intrauterine death (IUD) and antepartum haemorrhage (APH) but with no other systemic disease, was referred to our tertiary care hospital after vaginal delivery in a peripheral hospital. In the postpartum period she had nausea, vomiting, headache, blurring of vision, altered sensorium, high blood pressure of 170/100 mmHg and a pulse rate of 92 beats/min. Empiric antibiotics were started but urine and blood cultures showed negative results at a later date. Serum hemoglobin level was 7 g/dl, hematocrit of 26.9%. Injectable iron was started. Her kidney function tests showed blood urea 80 mg/dl and creatinine 4.5mg/dl. Anticipating need for dialysis the viral markers were sent which were negative. Aggressive hydration was done and then patient was sent for CT scan of head, which showed hypodense lesions involving occipital region (Figure 1) suggesting edema. MRI brain confirmed the diagnosis of PRES as shown in Figure 2.
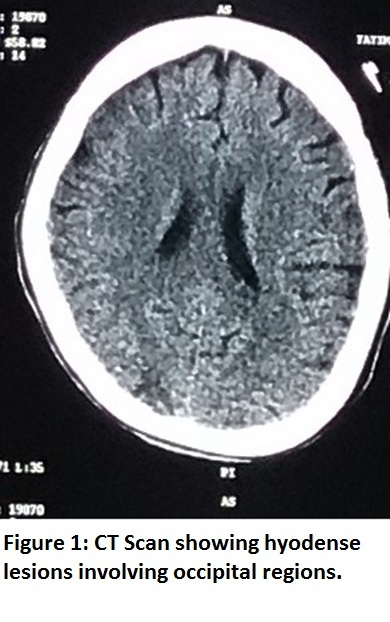
Figure 1: CT Scan showing hypodense lesions involving occipital regions
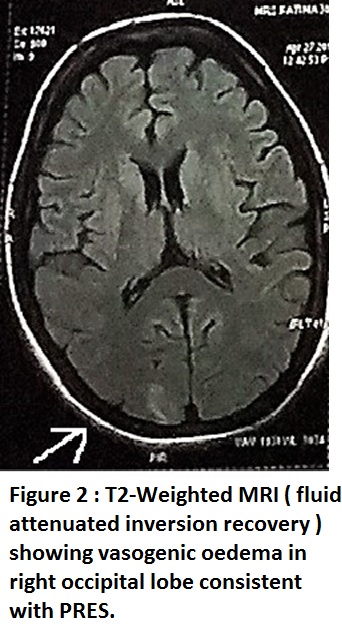
Figure 2: T2-Weighted MRI (fluid attenuated inversion recovery) showing vasogenic edema in right occipital lobe consistent with PRES
The patient was put on regular antihypertensives and injection mannitol for vasogenic edema. The vitals were gradually controlled and kidney functions also returned back to normal within 5 days period. The MRI brain repeated after 2 weeks showed complete resolution of neuro-radiological features of PRES.
DISCUSSION
The lesions of PRES are best visualized with MRI T2 weighted images at the height of symptoms. It characteristically shows diffuse hyper intensity selectively involving the parieto-occipital white mater. Occasionally the lesion may involve the grey mater. However, computed tomography can also be used satisfactorily to detect hypodense lesions of posterior leukoencephalopathy.4
The differential diagnosis of PRES is a broad one. Venous thrombosis or subdural or intracerebral or subarachnoid hemorrhages can also present with headache, seizures, reduced consciousness and focal neurological signs. It is important to consider the diagnosis of posterior circulation stroke because its treatment (urgent thrombolysis) and prognosis, both differ from those in PRES. Basilar artery thrombosis can present with progressive neurological deficits and can result in hemiparesis, coma and locked in syndrome.5
In our case, the patient had acute kidney injury due to antepartum haemorrhage, which was the cause for hypertension; and not due to preeclampsia or eclampsia which are commonly thought causes for hypertension in pregnancy, as the urinary protein or oedema were not present and there was no history of convulsions or hypertension. Immediate CT brain ruled out venous sinus thrombosis and cerebral hemorrhage. Although not 100% sensitive, CT may also demonstrate venous snus thrombosis, arterial ischemia or thrombosis.6
In PRES, the cause of acute hypertension are commonly acute kidney injury or eclampsia but can be seen in autonomic disturbances like Guillain-Barre Syndrome.7,8 Venous sinus thrombosis can be rapidly diagnosed by CT or MR venography. However MR venography could not be done because of its unavailability.
Our patient responded very well to antihypertensives and diuretics along with antibiotic coverage. The symptoms reverted within 5 days, MRI repeated after 2 weeks showed no residual findings.
The cause of PRES remains controversial but the most popular theory is that severe hypertension causes interruption of brain autoregulation. Uncontrolled hypertension leads to hyperperfusion and cerebral vessel damage, resulting in interstitial extravasation of proteins and fluids, causing vasogenic edema. An alternative theory is that PRES is a result of a systemic inflammatory state causing endothelial dysfunction. When blood pressure is high the vasoconstriction that occurs during autoregulation could exacerbate such a preexisting inflammatory endothelial dysfunction causing hypoxia and subsequent vasogenic edema.9 Rapid withdrawal of the trigger hastens the recovery, thus avoiding complications. Corticosteroids should theoretically improve vasogenic edema but there is no evidence of their use in PRES. No clinical trials have evaluated the management of PRES.6
Many studies have mentioned hemorrhage as major cause of pregnancy related acute kidney injury with PPH on the lead. Pregnancy is responsible for 15-20% AKI in developing countries. Our patient had APH which was probably the cause of AKI.10
CONCLUSION
It is important for the intensivist to be cognizant of this entity, as a delay in the diagnosis and treatment can result in permanent damage of the affected brain tissues. Early recognition of this brain disorder may eliminate the need for extensive, invasive investigations. Prompt treatment without delay carries a favourable prognosis without unnecessary repeated neuroimaging.
Conflict of interest: Nil
Author contribution: AC, DA – Concept, literature search, manuscript preparation
AG – Data acquisition, analysis
SSC – Manuscript review
REFERENCES
- AYH,Buonanno FS, Schrter PW, Le DA, Wang B, Gonzalez RG, Koroshetz WJ. Posterior Leukoencephalopathy without severe hypertension: utility of diffusion weighted MRI. Neurology 1998;51(5):1369-76 [PubMed]
- Pugliese S, Finocchi V, Borgia ML, Nania C, Della Vella B, Pierallini A, Bozzao A. Intracranial hypotension and PRES: case report. J Headache Pain 2010;11(5):437-40. [PubMed] [Free full text] doi: 10.1007/s10194-010-0226-z
- Hinchoy J, Chaver C , Appignani B, Breen J, Pao L, Wang A, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996;334:494-500 [PubMed] [Free full text]
- Akhvlediani R, Mogylevsky A, Contant S. Clinical report of posterior leukoencephalopathy syndrome. Georgian Med News 2008;154:22-6 [PubMed]
- Hobson EV, Craven I, Blank SC. posterior reversible encephalopathy syndrome: a truly treatable neurologic illness. Perit Dial int 2012;32:590-4 [PubMed] [Free full text] doi: 10.3747/pdi.2012.00152.
- Roth C, Ferbert A. The posterior reversible encephalopathy syndrome- what’s certain, what’s new? Pract Neurol 2011;11:136-44. [PubMed] [Free full text] doi: 10.1136/practneurol-2011-000010.
- Barikatte G, Gaber T, Eshieff NU. Posterior reversible encephalopathy syndrome as a complication of Guillain- Barre Syndrome. J Clin Neuro Sci.2010;17-924-6. [PubMed] doi: 10.1016/j.jocn.2009.11.009.
- Jorge S, Lopes JA, Dc Almeida E, Martins PM. Posterior reversible encephalopathy syndrome and chronic kidney disease. Nefrologia 2007;27:650. [PubMed] [Free full text]
- Bartynski W. Posterior reversible encephalopathy syndrome, Part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol 2008;29:1043-9. [PubMed] [Free full text] doi: 10.3174/ajnr.A0929
- Nafar MS, Shah AR, Warin IA, Reshi AR, Banday KA, Bhat MA, et al. Pregnancy related acute kidney injury: A single centre experience from the Kashmir valley. Indian J Nephrol 2008;18:159-61. [PubMed] [Free full text] doi: 10.4103/0971-4065.45291.
