
Sneha Raju, MD1, Pravin Ubale, MD2, Abhijit S. Nair, MD3
1Assistant professor, Dept. of Anesthesiology, LTMGH & LTMMC, Sion, Mumbai, (India);
E-mail: drsneharaju@gmail.com
2Associate Professor, Dept. of Anesthesiology, TNMC &BYL Nair Hospital, Mumbai (India); E-mail: drpravinubale@gmail.com
3Consultant Anesthesiologist, Basavatarakam Indo-American Cancer Hospital & Research Hospital. Hyderabad, (India); E-mail: abhijitnair95@gmail.com
Correspondence: Dr. Pravin Ubale, Anand Bhavan, B–16, TNMC & BYL Nair Hospital, Mumbai Central, Maharashtra, Mumbai-400011 (India) ; Tel: 9322211472; E-mail: drpravinubale@gmail.com
ABSTRACT
Background and Objective: Subclavian vein (SV) catheterization via infraclavicular approach is routinely done for multiple uses in operating rooms as well as in intensive care units in selected patients. The aim of this study was to evaluate the influence of shoulder position on central venous catheter (CVC) tip location during infraclavicular subclavian approach.
Methodology: A prospective observational study was conducted on 60 patients and included American Society of Anesthesiologist (ASA) physical status 1 and 2 patients in whom CVC was planned. Catheters were introduced either in neutral shoulder position or the shoulder was lowered during venipuncture and guide wire insertion. A post-operative chest x-ray was done to note any complications and catheter tip malposition.
Results: Demographic data was comparable between the two groups with respect to age, gender and weight. (P > 0.05). In one case in Group A, and two cases in Group B there was failure to puncture the vein but this was statistically insignificant (P = 0.554). Failure to thread the guidewire was seen in one case in each group with no statistical significance (P > 0.05) Statistical difference was noted in successful placement of CVC tip between the two shoulder position (P = 0.025).
Conclusion: The neutral shoulder position reduced the incidence of catheter misplacements during infraclavicular approach of right subclavian vein catheterization as compared to lowered shoulder position.
Key words: Central Venous Catheterization; Central Venous Catheters; Subclavian Vein;
Patient Positioning; Catheters
Citation: Raju S, Ubale P, Nair AS. A study to evaluate the influence of shoulder position on central venous catheter tip location during infraclavicular subclavian approach. Anaesth Pain & Intensive Care 2016;20(4):393-397
Received: 7 Sep 2016; Reviewed: 17 Oct, 27 Oct 2016; Corrected: 12 Nov, 9 Dec 2016; Accepted: 25 Dec 2016
INTRODUCTION
The history of central venous cannulation started in 1929 when Forssmann described the advance of a plastic tube to the heart by puncturing his own arm vein.1 In 1952, Sven-Ivar Seldinger developed an innovative technique for the percutaneous insertion of large bore catheters into blood vessels. The Seldinger technique for central venous catheter (CVC) placement is widely used in medical practice. The subclavian vein, long favored by surgeons,2-4 offers an alternative to the internal jugular vein for central venous access. It is associated with fewer infectious complications than the internal jugular vein route and remains accessible after localized thrombosis in internal jugular vein. A non-randomized study by Sandhu et al suggests that the arterial puncture is more frequent with the internal jugular approach whereas catheter malposition is more frequent with the subclavian approach, and the incidence of pneumothorax, hemothorax, and thrombosis are equivalent.5
Subclavian vein (SV) can be cannulated via the supraclavicular or an infraclavicular approach. Infraclavicular approach is the commoner approach for cannulating the SV for central venous access.6 During cannulation, shoulder position plays an important role in proper placement of CVC. Commonly used shoulder positions for cannulation are neutral and lowered positions.7,8 They produce a constant relation between the clavicle and the SV increasing the safety and reliability of SV puncture. We hypothesized that having a neutral shoulder position has a greater success rate of SV cannulation with infraclavicular approach instead of a lowered shoulder position. Therefore we designed and conducted this prospective randomized study to evaluate the influence of shoulder position on CVC tip location during right infraclavicular subclavian approach.
METHODOLOGY
This was a prospective randomized study conducted at a tertiary care teaching public hospital after obtaining the Institutional Ethics Committee approval and written and informed valid consent from the patients. Patients were randomly allocated into two groups using computer generated randomization list. Study was conducted over a period of one and a half years from September 2012 to March 2014. A total of 60 patients, aged 18-60 years, ASA physical status I and II undergoing elective major abdominal surgeries under general anesthesia were included in the study. Patient with bleeding diathesis, coagulopathy, chest deformity and infection at the puncture site were excluded. Monitoring with electrocardiogram, pulse oximeter and non-invasive blood pressure was instituted. Peripheral venous access was secured after which the patient was administered general anesthesia. Following tracheal intubation, with an appropriately sized tube infraclavicular right SV cannulation was done using the modified Seldinger technique. SCV cannulation was performed by an anesthesiologist with at least three year experience in performing SCV cannulation. The procedure was done under all aseptic condition taking universal precautions. The patients were placed in the supine position with arms kept by the side and the head in the neutral position with the operating table flat.
In Group A, the right shoulder was kept in the neutral position during venipuncture and guide wire insertion. In Group B, the right shoulder was pulled downward by an anesthesia post graduate student by firmly grasping and pulling the right wrist of the patient during venipuncture and guide wire insertion. After sterile preparation and draping, the skin was punctured using the puncture needle provided in the kit at a point just below the right clavicle lateral to the mid-clavicular line towards the suprasternal notch and the puncture needle was attached to a syringe with hub of the needle directed caudally and advanced until the clavicle was met. While maintaining a slight constant negative pressure, the needle was advanced under the inferior border of the clavicle until the right SV was punctured. After confirming flashback of non-pulsatile blood, the guidewire was advanced with the J-tip of the guidewire facing downward. Dilator was passed over the guidewire to slightly enlarge the tract. A triple lumen CVC (Arrow Company, 7.5 French) was then passed over the guidewire which was removed. After removing the guidewire, all ports of the central line were checked for free flow of blood. Once free flow was confirmed, suturing was done and a sterile dressing was applied over the area of insertion. If the first attempt was unsuccessful, the needle was slowly withdrawn under constant and slight negative pressure until the needle tip was in subcutaneous tissue and the needle was re-advanced in slightly cephalic or caudal direction.
Successful placement was considered when catheter tip was in distal SV or at the SV and right atrial junction. Catheter tips located in the ipsilateral internal jugular vein or in contralateral brachiocephalic vein were considered as misplacement. Postoperative chest radiographs were taken to check for pneumothorax and the location of the catheter tip.
Statistical analysis: Appropriate statistical tests (parametric and non-parametric) were applied on the data. A p-value of less than 0.05 was considered to be statistically significant. Sample size was calculated with the help of previous study.9 By comparison of proportion method sample size was calculated at 80% power and 5% α error. Minimum sample size was found to be 30 patients in each group. Qualitative and quantitative data were represented in form of frequency and percentage and mean ± SD and median and interquartile range (IQR) respectively. Association between qualitative variables was assessed by Chi-Square test with continuity correction for all 2 × 2 tables. Analysis of quantitative data between the two groups was done using unpaired t-test if data passed ‘normality test’ and by Mann-Whitney test if data failed the test. Results were graphically represented where deemed necessary. SPSS version 17 was used for analysis. Microsoft Word and Excel were used for data representation.
RESULTS
We studied 60 patients with 30 each in group; Group A with the right shoulder kept in the neutral position and other group with shoulder in a lowered position. Our data analysis showed that demographic data were comparable between the two groups with respect to age, gender and weight (P > 0.05) (Table 1).
Table 1: Comparison of age and weight between two groups
| Variables | Group A | Group B | t-value | p-value |
| Age (years) | 40.67 ± 12.75 | 39.13 ± 11.76 | 0.484 | 0.630* |
| Weight (kg) ^ | 62.70 ± 9.37 | 63.57 ± 9.33 | -0.318 | 0.750* |
| Male : Female | 16 : 14 | 18 : 12 | > 0.05 |
*Not significant
Comparison between the two groups with respect to type of surgery showed no statistical significant difference (p = 0.718) (Table 2).
Table 2: Comparison on type of surgeries (P = 0.718)
| Surgery | Group A
(n) |
Group B
(n) |
Total |
| Craniotomy | 6 | 6 | 12 |
| Exploratory laparotomy | 11 | 15 | 26 |
| Decompression craniotomy | 7 | 5 | 12 |
| Whipples surgery ^ | 2 | 2 | 4 |
| Hepatico-jejunostomy ^ | 1 | 2 | 3 |
| Abdomino-perineal resection ^ | 1 | 0 | 1 |
| Esophageal surgery ^ | 1 | 0 | 1 |
| Triple bypass surgery ^ | 1 | 0 | 1 |
| Total | 30 | 30 | 60 |
There was only one case in Group A and two cases in Group B where there was failure to puncture and this was statistically not significant (p = 0.554) (Graph 1). Successful cannulation was achieved in single attempt in 18 cases in Group A and 14 cases in Group B. Mean number of attempts was marginally high in Group B (1.73 ± 0.91) as compared to Group A (1.57 ± 0.86), though statistically this was not significant (p = 0.489).
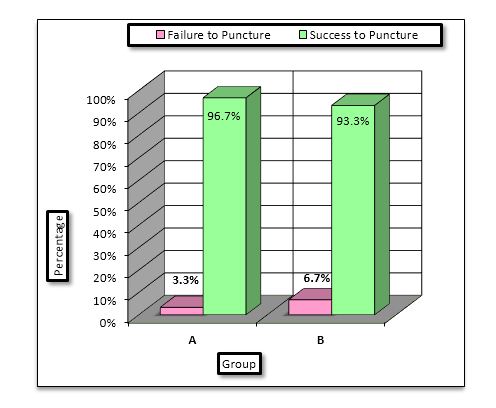
Graph 1: Comparison of failure to puncture
Failure to thread the guidewire was seen in one case in each group with no statistical significance noted p > 0.05 (Graph 2).
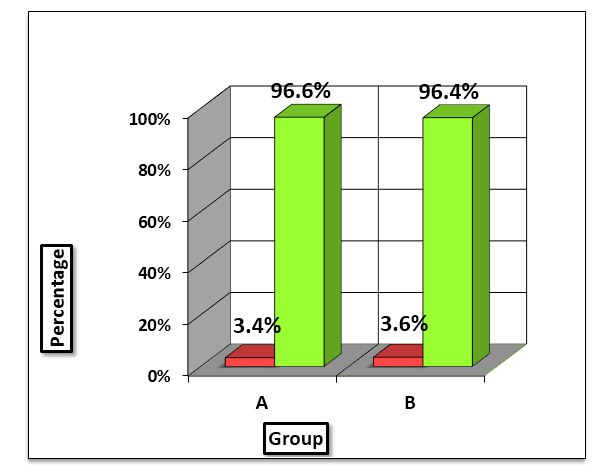
Graph 2: Comparison of failure to thread guidewire
There was no failure to thread the catheter over the guidewire in either group. The only complication we observed in both the groups was arterial puncture. Two patients in Group A and three patients in Group B had an arterial puncture. However, there was no statistical significance noted (p = 1.00).
Twenty-seven patients in Group A and twenty patients in Group B had successful placement of the CVC tip (catheter tip at the distal superior vena cava or at the right atrial junction) and this was statistically significant (p = 0.025) (Graph 3). One patient in Group A and three patients in Group B had the catheter tip placed in the ipsilateral internal jugular vein. Four patients in Group B had the catheter tip placed in contralateral brachiocephalic vein as compared to none in Group A which was statistically significant (p = 0.025) (Graph 3).
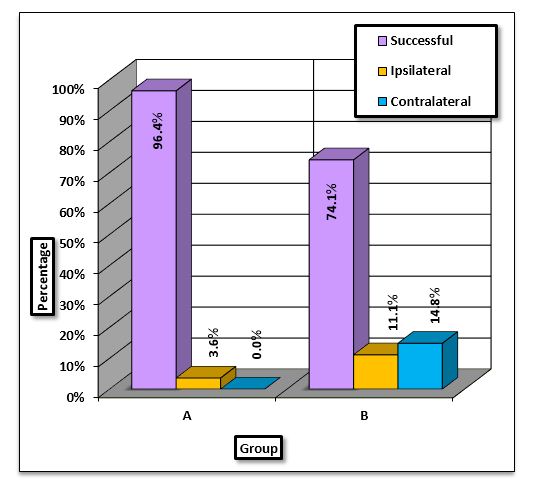
Graph 3: Comparison of placement of catheter in two groups
DISCUSSION
SV catheterization is a common practice amongst anesthesiologists, intensivists and emergency room physicians for major surgical procedures as well as for intensive care monitoring and rapid restoration of blood volume. Infraclavicular approach has been well established as a relatively safe method. However, there have been instances of malposition of the catheter tip in the ipsilateral IJV or contralateral brachiocephalic vein. In order to decrease the chance of aberrant catheter placement, various shoulder positions have been suggested. In our study we compared neutral versus shoulder lowered position for catheter tip placement in infraclavicular SCV catheterization. We observed that neutral position of the shoulder resulted in increased chances of successful placement of the CVC as compared to shoulder down position.
Kitagawa N et al9 conducted a study to observe spatial relations between the SV and surrounding structures using multislice computed tomography to determine optimal shoulder position for SV catheterization. Anatomical relations between the subclavian artery and vein were also observed. The subclavian artery lies behind and slightly superior to the path of the subclavian vein. Although the subclavian artery is in close contact with the SV in the up and neutral positions, the investigators observed that the tendency for contact between the subclavian artery and vein decreases at the clavicular head of the sternocleidomastoid muscle with a lowered shoulder position. This is because the SV undergoes a relatively greater inferior shift than the subclavian artery in the lowered shoulder position. A needle advanced along the undersurface of the clavicle usually enters the SV beneath the inner third of the clavicle, particularly near the clavicular head of the sternocleidomastoid. The risk of arterial puncture maybe reduced in lowered shoulder position.
In 2011, Kang M et.al 10 conducted a prospective study to assess the influence of the shoulder position on proper placement of right infraclavicular subclavian catheters. It was hypothesized that with the shoulder pulled downwards, the angle between the internal jugular and subclavian veins may increase, directing subclavian catheters into the internal jugular vein. Patients who required subclavian CVC for major neurosurgical and thoracic procedures were randomly divided into two groups: neutral (n = 180) vs lowered (n = 181) shoulder position. In this study there was one case in neutral group and two cases in shoulder lowered group where SV could not be punctured which was comparable to our observations Similarly catheter tip misplacement was observed in only 2 cases out of 173 in neutral shoulder group as compared to 14 out 173 patients in shoulder lowered position which was comparable to our study. A possible explanation can be that the shoulder lowered position decreases the angle between the SV and brachiocephalic vein which may direct the SV into ipsilateral IJV. Also there is increase in the angle between right brachiocephalic and left brachiocephalic which directs the catheter into the contralateral brachiocephalic vein.
In 2013, Kim et.al11 performed a study in which they hypothesized that the neutral shoulder position would not be inferior to the retracted shoulder position with regards to success rate of subclavian venous catheterization. A total of 362 patients who underwent elective surgery were randomly assigned to two groups: those who underwent subclavian venous catheterizations in the neutral shoulder position (neutral group, n = 181) or in the retracted shoulder position (retracted group, n = 181). Failure to puncture the vein was observed in two cases in retracted group and one case in the neutral group which was similar to our study. Also in similar study successful catheter placement was observed in total of 347 patients with 173 patients belonging to neutral group and 174 to the retracted group. This was in contrast to our study where there were more successful placements in Group A (neutral) than in Group B.
In 1987, Jesseph JM et.al12 studied the potential effect of various body positions on SV catheterization using gross anatomic dissection and magnetic resonance imaging. Findings showed that traditional recommendations for patient positioning with the shoulders retracted can lead to distortion of the SV anatomy and make successful cannulation more difficult. They suggested positioning the patient flat with the head and shoulders in a neutral position to improve the chances of successful catheter placement.
LIMITATIONS
Our study has a few limitations such as small sample size. There might be small variations in skill of the anesthesiologist performing the procedure. The study was not blinded and this may have introduced bias. Our study involved right SV cannulation only. Further studies are required to ascertain the ideal vein i.e. right versus left SV cannulation. Intravascular volume status was not assessed which is ideally done by sonographic evaluation of inferior vena cava. Patients for elective laparotomy undergo bowel preparation due to which they become dehydrated and hypovolemic. Cannulation might be difficult if done by blind and landmark technique thereby making the procedure difficult and thus leading to complications like pneumothorax. Inclusion criteria should include type of surgery and assessment of intravascular volume status (IVC assessment by USG).
CONCLUSION
We conclude that the neutral shoulder reduces the incidence of catheter misplacements during infraclavicular approach of the right SV catheterization as compared to shoulder lowered position.
Acknowledgment: We express our sincere thanks to our Head of Department and Ethics committee members for making this study possible
Conflict of Interest: None
Authors’ Contribution: SR: conduction of the study; PU: concept; AN: manuscript editing
REFERENCES
- Meyer JA. Werner Forssmann and catheterization of the heart, 1929.Ann Thorac Surg. 1990 Mar;49(3):497-9. [PubMed]
- Linos DA, Mucha P, Van Heerden JA. Subclavian vein: A golden route. Mayo Clin Proc. 1980;55(5):315–321. [PubMed]
- Thompson EC, Calver LE. Safe subclavian vein cannulation. Am Surg. 2005;71:180–183. [PubMed]
- Ruesch S, Walder B, Tramer MR. Complications of central venous catheters: Internal jugular versus subclavian access – A systematic review. Crit Care Med. 2002;30:454–460. [PubMed]
- Sandhu NS. Transpectoral ultrasound-guided catheterization of the axillary vein: An alternative to standard catheterization of the subclavian vein. Anesth Analg. 2004;99:183–187. [PubMed]
- Tan BK, Hong SW, Huang MH, Lee ST. Anatomic basis of safe percutaneous subclavian venous catheterization. J Trauma 2000;48:82-6. [PubMed]
- Boyd R, Saxe A, Phillips E. Effect of patient position upon success in placing central venous catheters. Am J Surg 1996;172:380-2. [PubMed]
- Fortune JB, Feustel P. Effect of patient position on size and location of the subclavian vein for percutaneous puncture. Arch Surg 2003;138:996-1000. [PubMed] [Free full text]
- Kitagawa N, Oda M, Totoki T, Miyazaki N, Nagasawa I, Nakazono T.et al. Proper shoulder position for subclavian venipuncture: a prospective randomized clinical trial and anatomical perspectives using multislice computed tomography. Anesthesiology. Dec 2004;101(6):1306-12. [PubMed] [Free full text]
- Kang M, Ryu HG, Son IS, Bahk JH. Influence of Shoulder position on central venous catheter tip during infraclavicular subclavian approach. British Journal of Anesthesia 2011;106(3):344-7. doi: 10.1093/bja/aeq340. [PubMed] [Free full text]
- Kim HJ, Jung SH, Min J, Hong DM, Jeon Y, Bahk JH. Comparison of the neutral and retracted shoulder positions for infraclavicular subclavian venous catheterization: a randomized, non-inferiority trial. Br J Anesth. Aug 2013;111(2):191-6. doi: 10.1093/bja/aet026. [PubMed] [Free full text]
- Jesseph JM, Conces DJ, Augustyn GT. Patient positioning for subclavian vein catheterization. Arch Surg. 1987;122:1207–1209. [PubMed] [Free full text]
