
Yashpal Singh, MD1, Shashi Prakash, MD1, Neeraj Kumar, MD2, Atul Kumar Singh , MD1, Bikram Kumar Gupta, MD1, Ram Badan Singh, MD3
1Assistant Professor; 2Senior Resident; 3Professor
Department of Anesthesiology, Institute of Medical Sciences, BHU, Varanasi-221005, UP, India
Correspondence: Dr. Yashpal Singh, Assistant Professor, Department of Anesthesiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, UP, (India); Phone: 91-9918424416; E-mail: dryashacin1999@rediffmail.com
ABSTRACT:
Objective: Intraoperative transient chest discomfort/pain is a common problem during lower segment cesarean section (LSCS), incidence ranging from 30-60 %. Only a few drugs are available to treat it due to concerns regarding maternal and fetal safety. Fentanyl is commonly used but has limited or no availability in most of India especially in rural areas. So we planned this study to compare ketamine as alternative to fentanyl to treat this chest discomfort/pain.
Methodology: This prospective, randomized, double blind study was carried out on sixty patients aged above 18 years, of American Society of Anesthesiologist (ASA) grade I or II scheduled for elective LSCS under spinal anesthesia, who complained of chest discomfort/pain within 15 min of delivery of baby. The parturients were randomly divided into two groups. Group F to receive inj fentanyl 1 µg/kg and Group K to receive inj ketamine 0.25 mg/kg intravenously immediately after complaining of chest discomfort/pain. Duration of surgery, time of onset of pain, time required to relieve pain, hemodynamic parameters, adverse event and duration of postoperative analgesia were observed. The drugs were compared by using equivalence test; Two-One-Sided-Test (TOST).
Results: There was no difference in demographic profile and baseline parameter in both groups. After drug administration chest discomfort/pain was relieved in both groups effectively in 1.15 ± 0.83 min vs. 1.23 ± 0.48 min in Group F and Group K respectively, without any significant adverse event.
Conclusion: Low dose ketamine can be used as alternative to fentanyl for transient retrosternal chest discomfort/pain during LSCS.
Key words: Retrosternal chest discomfort; Fentanyl; Ketamine
Citation: Singh Y, Prakash S, Kumar N, Singh AK, Gupta BK, Singh RB. A randomized, double blind study comparing fentanyl with ketamine for transient chest discomfort/pain during LSCS under spinal anesthesia. Anaesth, Pain & Intensive Care 2017;21(1):73-78
Received: 10 Jul 2016; Reviewed: 4, 11, 14, 20 Sep 2016, 11 Apr 2017; Corrected: 8, 13 Sep 2016, 11, 12 April 2017; Accepted: 12 April 2017
INTRODUCTION :
It has been observed that pain that occurs during lower segment cesarean section (LSCS) under spinal anesthesia have different etiology and occur at various stages of LSCS. Pain during LSCS can occur at the following points; 1- skin incision, this indicates an extremely poor level of regional anesthesia; 2 – peritoneal incision, this occurs prior to the uterine incision; exteriorization of the uterus; 3 – traction on the uterosacral ligaments or bladder; 4 – swabbing of the paracolic gutters; 5 – shoulder tip pain, this may be related to blood or amniotic fluid irritating the diaphragm (referred pain from the phrenic nerve, C3-C5); and 6 – chest pain, rarely this may be accompanied by ECG changes.1,2 The cause of chest discomfort/pain is unknown although small venous air emboli or coronary artery/ esophageal spasm/reflux have been suggested. Chest discomfort/pain usually occurs immediately after delivery of baby. The treatment options are limited, intravenous fentanyl /alfentanil /tramadol/ketamine or a 50:50 mixture of oxygen and nitrous oxide (Entonox) or 0.8% sevoflurane by anesthesia machine.3,4
Acute pain consists of basal or background pain with spikes of more intense pain layered on top of this background. The basal or background pain that can fluctuate over time is called breakthrough pain.5 Breakthrough pain, related to some specific activity is known as incidental pain. There is no literature addressing treatment of incidental pain occurring on operating table immediately after cesarean section. Intravenous opioids are well studied for intra-operative or postoperative pain relief but limited availability of short acting opioids like fentanyl or alfentanil, especially in rural/remote areas of developing countries prevents their use. Ketamine is well known and popular in every place, including rural areas. There is paucity of literature to treat this type of pain. So we planned this study to compare ketamine as an alternative to fentanyl for effectiveness to relieve chest discomfort/pain during LSCS.
METHODOLOGY:
After approval from hospital ethical committee, and informed consent, 60 patients aged above 18 years, of American Society of Anesthesiologist (ASA) grade I or II scheduled for elective LSCS under spinal anesthesia, and who complained of intra-operative chest discomfort/pain were included in this prospective, randomized-controlled, double-blinded trial. Patients with history of hypertension, ischemic heart disease, rheumatic heart disease, reflux esophagitis, disarranged hepatic or renal function, head trauma, psychiatric diseases, and sensitivity to studied drugs or contraindication to spinal anesthesia were excluded from the study.
All patients were randomly assigned to two equal groups. Randomization was done by an investigator involved in drug administration and data collection. Concealment was done via the sealed opaque envelope technique. Data analysis was carried out by another investigator blinded to group allocation. Patients complaining of chest discomfort/pain within 15 min after delivery of baby were included in the study. Group F to receive inj fentanyl 1 µg/kg and Group K to receive inj ketamine 0.25 mg/kg IV immediately after complaining of chest discomfort/pain. Duration of surgery, time of onset of pain, time required to relieve pain, hemodynamic parameters, adverse events were observed.
Premedication included tab ranitidine (150 mg), and tab metoclopramide (10 mg) administered orally on the evening before surgery and 2 h before the scheduled procedure. On arrival to the operative room, monitors were placed and baseline parameters recorded. All patients were preloaded with lactated ringer solution (15 ml/kg) via 18 G peripheral
IV catheter. Before the commencement of spinal anesthesia, patients were explained about the chest discomfort/pain. In the lateral decubitus position under standard aseptic precautions, using a midline approach lumbar puncture was performed at L3-L4 or L4-L5 intervertebral space by 25 gauge Quincke spinal needle (BD, Gurgaon, Haryana, India). Having confirmed the free flow of cerebrospinal fluid through the spinal needle, Bupivacaine (heavy) 2.5 ml solution was injected intrathecally over a period of 10–15 sec. and patients were turned to the supine position. Surgery was not allowed till bilateral sensory block reaches up to T4 level. Just after delivery of baby all patients received oxytocin 5 units slow IV over 2-3 min and 10 units in 500 ml of dextrose normal saline slow infusion over 3-4 hours according to protocol. Any episode of hypotension (systolic blood pressure < 90 mmHg or > 25% below baseline) was managed by ephedrine (5 mg) and an additional fluid bolus of ringer lactate solution. Bradycardia (< 50 beats/min) was managed by inj atropine 0.5 mg IV bolus.
Statistical analysis: The statistical analysis was performed with Minitab 17 statistical software by using Two One-Sided Test (TOST) for equivalence, for comparison of hemodynamic parameters and time required to relieve chest discomfort. In this study we wanted to prove that ketamine could be safely used in place of fentanyl, and was not significantly inferior to fentanyl; thus it was a non-inferiority study. TOST is the appropriate test for this study which can prove that two means are sufficiently equivalent (Figure 1).
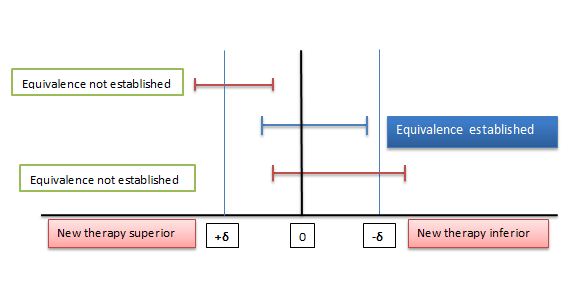
Figure 1: Two One-Sided Test procedures (TOST) and the equivalence margin in equivalence testing. δ: Equivalence margin
The equivalence margin, denoted by δ is the important feature of equivalence or non-inferiority test. Equivalence margin of difference is set as 20% of mean value. If 90% confidence interval is within the equivalence interval, we can claim equivalence. If greater of the two p-values is < 0.05 then we claim that two means are same
RESULTS:
All 60 patients completed the study successfully (Figure 2). The study groups were comparable in terms of demographic profile, baseline hemodynamic variables, ASA status and the duration of surgery (Table 1).
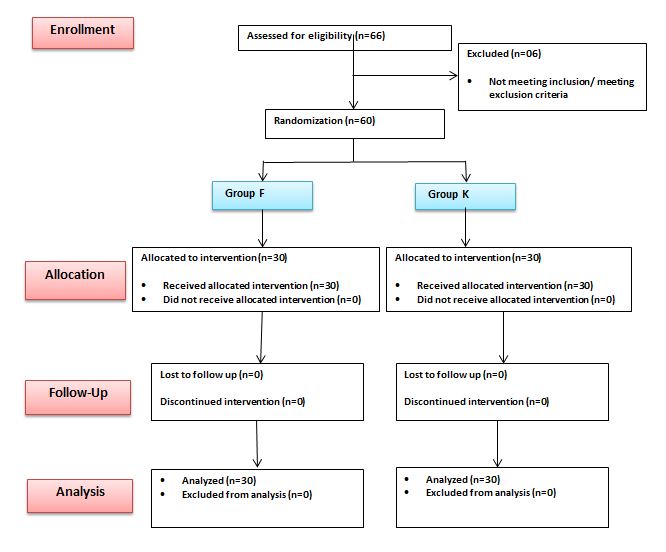
Figure 2: Flow chart of patients studied
Table 1: Demographic profile and baseline parameter between two groups.
| Parameter | Group F | Group K | p value |
| Age (year) | 31.24 ± 3.12 | 30.16 ± 2.32 | 0.134 |
| Body weight(kg) | 53.30 ± 7.07 | 53.35 ± 10.0 | 0.982 |
| Parity | 1.77 ± 0.78 | 1.84 ± 0.94 | 0.754 |
| No. of Previous LSCS | 1.87 ± 0.83 | 1.69 ± 0.56 | 0.329 |
| Duration of surgery(min) | 66.50 ± 16.8 | 66.25 ± 14.94 | 0.951 |
| ASA I/II | 13/17 | 12/18 | 1.00 |
| Baseline heart rate (beats/min) | 92.80 ± 8.65 | 94.12 ± 7.34 | 0.526 |
| Baseline systolic blood pressure (mmHg) | 128.16 ± 10.84 | 127.20 ± 11.13 | 0.736 |
| Baseline diastolic blood pressure (mmHg) | 83.33 ± 12.21 | 84.63 ± 11.39 | 0.641 |
Data are presented as mean ± SD. p value <0.05 considered as significant. LSCS= Lower segment cesarean section, ASA= American Society of Anesthesiologist, SD=Standard deviation
Maximum number of patients developed chest discomfort/pain after administration of oxytocin (about 50%) in both groups followed by time between peritoneal incision and delivery of baby (Table 2).
Table 2: Timing of Retrosternal chest discomfort/pain.
| Timing of Pain | Group F | Group K |
| At peritoneal incision (PI) | 03 (10%) | 02 (6.67%) |
| Between PI and delivery of baby (DB) | 05 (16.67%) | 07 (23.33%) |
| Within 5 min of oxytocin administration | 16 (53.33%) | 14 (46.67%) |
| After 5 min of oxytocin administration | 05 (16.67%) | 06 (20%) |
| At time of peritoneal closure | 01 (3.33%) | 01 (3.33%) |
Data are presented as occurrences or percentage.
After intravenous injection chest discomfort/pain was relieved in 1.15 ± 0.83 min in Group F, while in 1.23 ± 0.48 min in Group K. TOST analysis shows that two means are not equal (Table 3), but this difference 0.08 min (4.8 second) between two groups was not clinically significant.
Table 3: Time required relieving chest discomfort/pain after drug administration
| Parameter | Group F | Group K | Equivalence interval | 90% confidence interval | p value |
| Time (minutes) | 1.15 ± 0.83 | 1.23 ± 0.48 | ± 0.23 | -0.21 0.37 | 0.04 0.19 |
Data are presented as Mean ± SD. SD=Standard deviation. Confidence interval is the outside the equivalence interval and greater of two p value is 0.19, so two means are not equivalent.
There was significant fall in heart rate and systolic blood pressure from baseline value after subarachnoid block in both groups but intergroup comparison shows that two means are equal (Table 4). At onset of chest discomfort/pain, there were transient increase in heart rate and blood pressure from baseline value in both groups but intergroup comparison shows that means are equal (Table 4). After intravenous fentanyl, heart rate and mean arterial blood pressure approaches towards baseline but in ketamine group, heart rate and mean arterial blood pressure remain higher but two means are equal and statistically comparable (Table 5).
Table 4: Systolic blood pressure at different time intervals.
| Systolic blood pressure | Group F | Group K | Equivalence interval | 90% confidence interval | p-value |
| Baseline | 122.16 ± 10.84 | 121.20 ± 11.13 | ± 24.43 | -5.70 3.78 | 0.00 0.00 |
| 5 min after subarachnoid block | 103.27 ± 8.83 | 102.12 ± 8.12 | ± 20.65 | -4.81 2.51 | 0.00 0.00 |
| At onset of chest discomfort/pain | 128.31 ± 9.45 | 127.81 ± 10.13 | ± 25.66 | -4.73 3.73 | 0.00 0.00 |
| 5 min after drug administration | 118.26 ± 9.12 | 130.45 ± 8.98 | ± 23.65 | 8.82 16.09 | 0.00 0.00 |
| 10 min after drug administration | 114.45 ± 8.86 | 125.12 ± 9.24 | ± 22.89 | 6.76 14.58 | 0.00 0.00 |
| 15min after drug administration | 116.37 ± 7.98 | 120.23 ± 8.54 | ± 23.27 | 0.29 7.43 | 0.00 0.00 |
| Postoperative recovery room | 117.68 ± 10.12 | 118.65 ± 9.87 | ± 23.54 | -3.34 5.28 | 0.00 0.00 |
Data are presented as mean ± SD. SD=Standard deviation. Confidence interval is the within the equivalence margin, so two means are equal.
Table 5: Mean Heart rate (per minute) at different time intervals and their comparison with baseline.
| Time Interval | Group F | Group K | Equivalence interval | 90% confidence interval | p value |
| Baseline | 92.80 ± 8.65 | 94.12 ± 7.34 | ± 18.56 | -2.14 4.78 | 0.00 0.00 |
| 5 min after subarachnoid block | 79.60 ± 9.69 | 82.15 ± 8.65 | ± 15.92 | -1.41 6.51 | 0.00 0.00 |
| At onset of chest discomfort/pain | 104.23 ± 8.23 | 106.34 ± 8.45 | ± 20.84 | -1.49 5.71 | 0.00 0.00 |
| 5 min after drug administration | 111.30 ± 8.22 | 118.62 ± 10.24 | ± 22.26 | 3.31 11.33 | 0.00 0.00 |
| 10 min after drug administration | 96.64 ± 8.24 | 99.46 ± 9.34 | ± 19.33 | -0.98 6.62 | 0.00 0.00 |
| 15 min after drug administration | 95.12 ± 7.35 | 96.12 ± 8.42 | ± 19.02 | -2.41 4.41 | 0.00 0.00 |
| Postoperative recovery room | 94.34 ± 6.26 | 96.58 ± 8.11 | ± 18.87 | -0.89 5.37 | 0.00 0,00 |
Data are presented as mean ± SD. SD=Standard deviation. Confidence interval is the within the equivalence margin, so two means are equal.
Adverse events e.g. hypotension, bradycardia were more common in fentanyl group while tachycardia, ECG changes and nausea/vomiting were more common in ketamine group, but the difference was statistically insignificant between two groups (Table 6).
Table 6: Side Effects
| Parameter | Group F | Group K |
| Hypotension | 6 (20) | 4 (13.33) |
| Bradycardia | 3 (10) | 1 (3.33) |
| Tachycardia | 2 (2.67) | 4 (13.33) |
| ECG changes | 8 (26.67) | 9(30) |
| Shivering | 3 (10) | 2 (2.76) |
| Nausea/Vomiting | 2 (2.67) | 4 (13.33) |
Data are presented as occurrences (percentage)
DISCUSSION:
Our study demonstrates that low dose ketamine can be used safely as alternative to fentanyl for relief of transient retrosternal chest discomfort/pain during LSCS.
We selected ketamine because of its easy availability in developing countries, short duration of action and proven analgesic effect at sub-anesthetic dose by various mechanisms.6-9 In gynecologic surgery, there are some studies which used ketamine in sub anesthetic dosage. Sen et al. reported that women who received ketamine (0.15 mg/kg) during spinal anesthesia for LSCS operation had declined diclofenac recruitment in the first day postoperatively.10 Kwok et al. in laparoscopic gynecologic surgery reported that reduced requirement to paracetamol in the first week postoperatively in women who received ketamine (0.15 mg/kg).11
There is significant association between oxytocin administration and chest discomfort; approximately 50% of patients develop chest discomfort within five minute of oxytocin administration. Oxytocin is routinely given after delivery of baby to initiate uterine contraction and to prevent excessive bleeding. It is a vasoactive peptide and receptors are located in uterus, heart and large vessels and produces intense vasoconstrictive effect on uterine, umbilical and coronary artery.12,13 It decreases systemic vascular resistance leads to hypotension and reflux tachycardia.14,15 Mismatch between oxygen supply and demand occurs due to combination of tachycardia, hypotension and coronary vasoconstriction that leads to myocardial ischemia and chest discomfort/pain.16,17 Rest of patients develop chest discomfort/pain may be due to traction on peritoneum, reflux esophagitis, amniotic fluid embolism or small venous micro embolism etc.
Chest discomfort/pain was relieved within two minutes of IV injection of fentanyl or ketamine although the two means are not equal but difference of 4.8 second are not clinically significant. Ketamine causes sympathetic stimulation that lead to increase in heart rate and blood pressure while fentanyl causes decrease in heart rate and blood pressure but statistically not significant and two means are equal.
Women in our study had no considerable side effects and ketamine was tolerated well. Ketamine had some side effects such as urine suppression, hallucination, nausea and vomiting in women.18 Similar to our study, Meer et al. reported that ketamine in anesthesia for cesarean section had lower side effects.19
LIMITATION:
Our study has three main limitations. First, patients and surgeon satisfaction was not checked. Second, we did not access the duration of postoperative analgesia. Third, sample size was small. These results may vary from investigations performed on other ethnic groups due to variations in pain or drug sensitivity.
CONCLUSION:
We conclude that low dose ketamine can be used as a good alternative to fentanyl for relief of transient intra-operative chest discomfort/pain during LSCS under spinal analgesia, without any significant adverse events.
Acknowledgement: We would like to thanks to all technical staff, without whom the study could not have been completed.
Conflict of Interest: None
Author contribution: All authors contributed in the conduct of study, literature search, data analysis and manuscript preparation and review.
REFERENCES:
- Moran C, Ni Bhuinneain M, Geary M, Cunningham S, McKenna P, Gardiner J. Myocardial ischaemia in normal patients undergoing elective caesarean section: A peripartum assessment. Anaesthesia 2001; 56:1051-8. [PubMed] [Free full text]
- Zakowski MI, Ramanathan S, Baratta JB, Cziner D, Goldstein MJ, Kronzon I, et al. Electrocardiographic changes during cesarean section: A cause for concern? Anesth Analg 1993; 76:162-7. [PubMed] [Free full text]
- Rosen M. Nitrous oxide for pain relief of labor pain: a systemic review. Am J Obstet Gynecol. 2002 May;186(5 Suppl Nature):S110-26.[PubMed]
- Yeo ST, Holdcroft A, Yentis SM, Stewart A. Analgesia with sevoflurane during labour: i. Determination of the optimum concentration. Br J Anaesth 2007; 98:105-9. [PubMed]
- Svendsen KB, Andersen S, Arnason S, Arnason S, Arner S, Breivik H, et al. Breakthrough pain in malignant and non-malignant diseases: a review of prevalence, characteristics and mechanism. Eur J Pain. 2005; 9:195–206. [PubMed]
- Joselyn AS, Cherian VT, Joel S. Ketamine for labour analgesia. Int J Obstet Anesth. 2010; 19:122–3. doi: 10.1016/j.ijoa.2009.07.004. [PubMed]
- Ganla KN, Deshmukh S, Bhide A, Desai S. Analgesia in labor by intermittent intravenous bolus ketamine. J Obstet Gynaecol. 2000;4:60–2
- Bauchat JR, Low-dose ketamine with multimodal postcesarean delivery analgesia: a randomized controlled trial, Int J Obstet Anesth. 2011; 20:3-9. doi: 10.1016/j.ijoa.2010.10.002. [PubMed]
- Heesen M1, Böhmer J, Brinck EC, Kontinen VK, Klöhr S, Rossaint R, et al. Intravenous ketamine during spinal and general anaesthesia for caesarean section: systematic review and meta-analysis. Acta Anaesthesiol Scand. 2015 Apr;59(4):414-26. doi: 10.1111/aas.12468. [PubMed]
- Sen S, Ozmert G, Aydin ON, Baran N, Caliskan E. The persisting analgesic effect of low-dose intravenous ketamine after spinal anaesthesia for caesarean section. Eur J Anaesthesiol. 2005; 22:518-23. [PubMed] [Free full text]
- Kwok RF, Lim J, Chan MT, Gin T, Chiu WK. Preoperative ketamine improves postoperative analgesia after gynecologic laparoscopic surgery. Anesth Analg. 2004; 98:1044-9. [PubMed]
- Gutkowska J, Jankowski M, Mukaddam-Daher S, McCann SM. Oxytocin is a cardiovascular hormone. Braz J Med Biol Res 2000; 33:625-33. [PubMed]
- Fortner CL, Manley ES Jr, Woodbury RA. Effects of synthetic oxytocin with and without preservatives upon coronary blood flow in the dog. J Pharmacol Exp Ther 1969; 165:258-66. [PubMed] [Free full text]
- Pinder AJ, Dresner M, Calow C, Shorten GD, O’Riordan J, Johnson R. Haemodynamic changes caused by oxytocin during caesarean section under spinal anaesthesia. Int J Obstet Anesth 2002; 11:156-9. [PubMed]
- Langesaeter E, Rosseland LA, Stubhaug A. Hemodynamic effects of oxytocin during cesarean delivery. Int J Gynaecol Obstet 2006; 95:46-7. [PubMed]
- Svanström MC, Biber B, Hanes M, Johansson G, Näslund U, Bålfors EM. Signs of myocardial ischaemia after injection of oxytocin: A randomized double-blind comparison of oxytocin and methylergometrine during caesarean section. Br J Anaesth. 2008;100:683-9. doi: 10.1093/bja/aen071. [PubMed]
- Chilvers JP, Cooper G, Wilson M. Myocardial ischaemia complicatingan elective Caesarean section. Anaesthesia 2003;58:822-3. [PubMed] [Free full text]
- Subramaniam K, Subramaniam B, Steinbrook RA. Ketamine as adjuvant analgesic to opioids: a quantitative and qualitative systematic review. Anesth Analg. 2004; 99:482-95. [PubMed]
- Meer FM, Downing JW, Coleman AJ. An intravenous method of anaesthesia for Caesarean section. II. Ketamine. Br J Anaesth.1973; 45:191-6. [PubMed]
