
Sapna Bansal*, Sachin Bansal*, Muskan Dogra**, Izan Khan**
*Assistant Professor; **Postgraduate trainee
MM Institute of Medical Sciences and Research (MMIMSR) Mullana (Ambala), Haryana (India)
Correspondence: Dr Sapna Bansal, 289, Durga Colony, Naraingarh, Ambala, Haryana (India); Cell: +9896633125; E-mail:drsapna10@gmail.com
ABSTRACT
Cannulation of the subclavian vein (SCV) has been associated with some of the inherent risks. Post procedure chest x-ray is routinely done to confirm correct position and rule out any complication. Malpositioning of the CVC is although common but is a serious complication of central line placement. We discuss such a case of malpositioned CVC into left subclavian vein through right sided subclavian approach.
Key Words: Catheterization, Complications; Malpositioning; Catheterization, Central Venous/methods; Electrocardiography
Citation: Bansal S, Bansal S, Dogra M, Khan I. A malpositioned central venous catheter. Anaesth Pain & Intensive Care 2015;19(1):54-56
INTRODUCTION
Central vein cannulationis a very common procedure done now a days, done either through right internal jugular or right subclavian vein. It is often a successful and uncomplicated procedure. The reported incidence of complications during subclavian vein puncture varies from 1.8%1 to 9.3%.2 Malpositioning of CVC is one of the complications. Most commonly it gets directed to ipsilateral internal jugular vein (IJV), but rarely it may travel into contralateral subclavian vein. Here we present a case of malpositioned central venous catheter into contralateral subclavian vein.
CASE REPORT
A 34 years old ASA PS-1 female patient with body mass Index 40 was posted for laparoscopic cholecystectomy. Multiple attempts at peripheral vein cannulation failed due to poor visualisation of the veins through the excessive fat, so central venous access through right subclavian vein was decided.
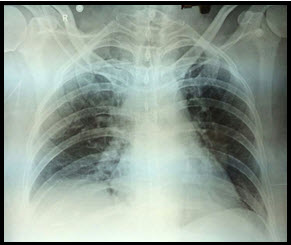
A 15 cm, 7 Fr triple lumen central venous catheter was inserted into the right subclavian vein using the Seldinger technique on first attempt without difficulty. A good back flow of blood was confirmed. Central line was secured and taped. A portable check x-ray chest was ordered, which revealed the malposition of central venous catheter into the left subclavian vein (Figure 1). The fluid infusion was terminated and the catheter was reinserted correctly through right IJV.
Figure 1: Central venous catheter seen malpositioned through left subclavian vein
DISCUSSION
The subclavian vein is well suited for cannulation because it is a large vessel (with diameter of 20 mm) that runs a fixed course. The major concern with subclavian vein is the risk of pneumothorax, but this is not a common occurrence.
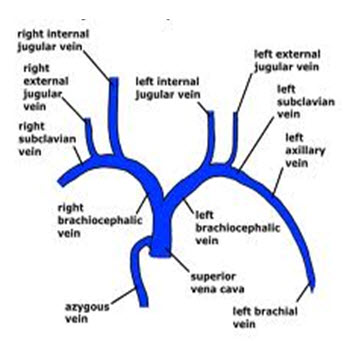
A properly placed subclavian catheter should run parallel to the shadow of superior vena cava and the tip of the catheter should be at or slightly above the third anterior intercostal space. The most commonly occurring malposition is into the IJV (60-70%)3. Other common sites include azygos vein, left superior intercostal vein and thymic vein. The contralateral subclavian vein is the most unusual site for migration of catheter. In our case guide wire inserted in the right subclavian vein passed through right brachiocephalic vein and instead of entering through superior vena cava, entered into the left brachiocephalic vein, and finally positioned into left subclavian vein (Figure 2).
Figure 2: Major veins superior to the heart
Various studies have explored the possible reasons for malposition of CVC. It could be most commonly because of change in the orientation of the J tip of the guide wire during the procedure.4 Final position of the catheter tip depends upon the course the guide wire takes. This error can be minimised by keeping the J tip of guide wire diverted caudad. Other factors are excessive length of the guide wire inserted and the venous route selected for puncture. Some authors recommend the upper limit of length of guide wire introduced upto 18 cm5 while others limit the length of CVC to 16.5 cm or ≤ 20 cm,6 but in such cases chances of malposition are as high as 45% requiring repositioning.7
The head or shoulder position appears to be important for the CVC direction during the infraclavicular subclavian approach.8-10 Turning the head away from the needle puncture site increases the angle of the SCV and IJV and causes malpositioning in the IJV.8,10 Lowering the shoulder position reduces the angle between the SCV and innominate vein, and increases the incidence of catheter misplacement into the ipsilateral IJV.9,10 In our case subclavian venous cannulation was performed with the head and shoulders in a neutral position.
The IJV occlusion test (applying external pressure on the IJV for approximately 10 seconds in the supraclavicular area and observing the changes in the CVP and its waveform pattern) rapidly detects the misplacement of subclavian vein catheter into the IJV. However, it does not detect any other misplacement.11
Another method to ensure successful correct placement is the use of real time ultrasound guided CVC insertion. With the ultrasound guided technique, the direction of needle is pointed along the long axis of the SCV, facilitating proper guide wire advancement. Other advantage is that it provides visualization of the vein and its anatomical variation, improves success rate and decreased number of venipuncture attempts and complications associated with it, but its role to direct insertion of CVC is controversial.
Studies have shown that ECG monitoring while performing the procedure can place the CVC tip in correct position in 92% of cases while monitoring change in configuration of p wave. In our case ECG monitoring was done throughout the procedure which didn’t show any change in pattern.
Although usually without any serious risks to the patient, aberrant placement of a subclavian venous catheter tip may result in incorrect central venous pressure readings or complications like erosion and thrombosis.
In conclusion, newer techniques like USG guided placement and endocavitary ECG to guide placement into SVC are available and should be used. Fluoroscopy provides a real time alternative to confirm the correct position of the guide wire and the catheter. However, there is no replacing the time tested confirmatory chest x-ray which still remains the easiest method to confirm the catheter position and must always be done.
REFERENCES
- Malatinsky J, Kudilic T, Májek M, Sámel M. Misplacement and loop formation of central venous pressure catheters. Acta Anaesth Scand 1976;20:237-47. [PubMed]
- Dietel M, McIntyre JP. Radiographic confirmation of site of CVP catheters. Can J Surgery 1971;14:42-52. [PubMed]
- Ambesh SP, Pandey JC, Dubey PK. Internal jugular vein occlusion test for rapid diagnosis of misplaced subclavian vein catheter into the internal jugular vein. Anesthesiology 2001;95:1377-9. [PubMed]
- Tripathi M, Dubey PK, Ambesh SP. Direction of the J-tip of the guidewire, in seldinger technique, is a significant factor in misplacement of subclavian vein catheter: a randomized, controlled study. Anesth Analg 2005;100:21-4. [PubMed]
- Andrews RT, Bova DA, Venbrux AC. How much guidewire is too much? Direct measurement of the distance from subclavian and internal jugular vein access sites to the superior vena cava-atrial junction during central venous catheter placement. Crit Care Med 2000;28:138-42. [PubMed]
- McGee WT, Ackerman BL, Rouben LR, Prasad VM, BandiV, Mallory DL. Accurate placement of central venous catheters: a prospective, randomized, multicenter trial. Crit Care Med 1993;21:1118-23. [PubMed]
- Anish M Joshi, Guruprasad P Bhosale, Geeta P Parikh. Optimal positioning of right- sided internal jugular venous catheters: Comparison of intra-atrial electrocardiography versus Peres’ formula. Ind J Crit Care 2008;12:10-14. [PubMed] [Free full text] doi: 10.4103/0972-5229.40943.
- Jung CW, Bahk JH, Kim MW, Lee KH, Ko H. Head position for facilitating the superior vena caval placement of catheters during right subclavian approach in children. Crit Care Med 2002;30:297–299. [PubMed]
- Kitagawa N, Oda M, Totoki T, Miyazaki N, Nagasawa I, Nakazono T, Tamai T, Morimoto M. Proper shoulder position for subclavian venipuncture: a prospective randomized clinical trial and anatomical perspectives using multislice computed tomography. Anesthesiology 2004;101:1306–1312. [PubMed]
- Boon JM, van Schoor AN, Abrahams PH, Meiring JH, Welch T, Shanahan D. Central venous catheterization – an anatomical review of a clinical skill – part1: subclavian vein via the infraclavicular approach. Clin Anat 2007;20:602–611. [PubMed]
- Ambesh SP, Panday JC, Dubey PK. Internal jugular vein occlusion test for rapid diagnosis of misplaced subclavian vein catheter into the jugular vein. Anesthesiology. 2001;95:1377-9. [PubMed]
Rothschild JM. A systemic approach to teaching insertion of a central venous line. Arch Surgery 1999;134:738-740
