
Sandeep Kumar Kar1, Dipanwita Das2, Chaitali Sen Dasgupta3
Assistant Professor; Post-Doctoral Trainee; Professor
Department of Cardiac Anesthesiology, Institute of Post Graduate Medical Education & Research, Kolkata, (India)
Correspondence: Dr. Sandeep Kumar Kar, Assistant Professor, Department of Cardiac Anesthesiology, Institute of Post Graduate Medical Education and Research, A.J.C. Bose Road, Kolkata, (India); E-mail: sndpkar@yahoo.co.in
ABSTRACT
Dislodgement of coronary stent-balloon catheter before deployment during percutaneous coronary intervention though rare but life threatening complication. A 47-year-old male presented with history of angina for two years. Angiography revealed that there was a stenosis (90%) in the left anterior descending (LAD) artery and significant plaque in the circumflex artery. During PTCA a stent-balloon was dislodged in left main coronary artery (LMCA). Under cardiopulmonary bypass, with cardioplegic arrest, the stent-balloon-catheter was extracted through coronary arteriotomy with repair of ruptured LMCA. Coronary revascularization was done with reversed saphenous vein grafts to the LMCA and D1 coronary arteries.
Key words: Cardiac surgery; Cardiopulmonary bypass; Angiography; Coronary artery disease; Induced heart arrest; Cardioplegia
Citation: Kar SK, Das D, Dasgupta CS. A complication of coronary angioplasty leading to surgical emergency: a case report. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S154-S157
Received: 29 March 2016; Reviewed: 14 April 2016; Corrected & Accepted: 16 August 2016
INTRODUCTION
Percutaneous coronary stenting procedure for coronary artery disease is common but can sometimes result in life threatening complications. Balloon angioplasty can lead to different catastrophic complications like acute stent thrombosis, coronary perforations and dissection of coronary arteries.1,2 Severe dissection with abrupt closure can cause even death of the patient. Recently the authors have encountered a case in which coronary angioplasty balloon got stuck in the left main coronary artery (LMCA) in a completely dilated stent during angioplasty.
CASE REPORT
A 47-year-old, diabetic, hypertensive, chronic smoker was presented with exertional chest pain for last 2 years. He had family history of hypertension and diabetes. His resting electrocardiogram (ECG) revealed sinus rhythm and T-wave inversion in leads V4-V6. The transthoracic echocardiogram showed left ventricular (LV) relaxation abnormality and ejection fraction of 48%. Coronary angiography was done that showed significant plaque in the circumflex coronary artery proximal to the origin of first obtuse marginal branch (OM1) and significant lesion in the left anterior descending artery (LAD) with 90% obstruction in just after origin of 1st diagonal branch (D1).
Patient was on beta-blocker, isosorbide di-nitrate, clopidogrel and aspirin. Pre-procedure pulse rate was 70/min, noninvasive blood pressure 140/90 mmHg, and SpO2 100% on room air. After insertion of right femoral sheath, guide wire was inserted. An angioplasty balloon catheter was railroaded over it to place the stent at LAD after balloon dilatation. But accidentally following balloon dilatation, it could not be deflated and was impacted in the LMCA. Patient was complaining of severe substernal pain that was radiating to the back, followed by severe dyspnea and profuse sweating and restlessness. Patient’s vitals started deteriorating and BP fell to 90/60 mmHg. ECG revealed different types of arrhythmias and ST segment elevation in all anterior leads. Multiple attempts were made to deflate the balloon and to remove it but failed. Fluoroscopic angiography showed the partially inflated balloon in the LMCA and there was leakage of dye from LMCA suggesting LMCA rupture (Figures 1 to 4).
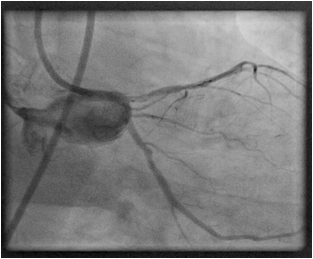
Figure 1: spillage of dye suggesting LMCA rupture
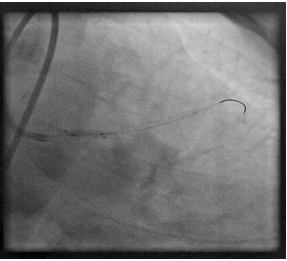
Figure 2 : Balloon in LMCA
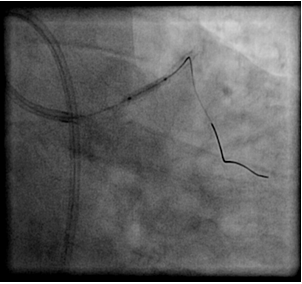
Figure 3: showing partially inflated balloon
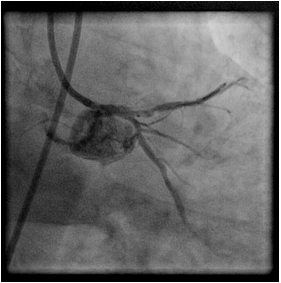
Figure 4: spillage confirms balloon rupture in LMCA
Due to rapidly deteriorating hemodynamic parameters of the patient, it was decided to shift the patient for emergency surgical intervention. Immediately the patient was shifted to cardiothoracic & vascular surgery operating room. Noradrenaline infusion was used to maintain blood pressure and the patient was posted for life saving coronary revascularization surgery.
Under cardiopulmonary bypass (CPB) the aorta was cross-clamped and heart was arrested with retrograde cardioplegia. The partially inflated balloon was removed out by coronary arteriotomy and the ruptured part of LMCA was repaired. LAD and D1 were re-vascularised with reversed saphenous vein grafts. After weaning from CPB, there was non-sustained ventricular arrhythmia; controlled by lignocaine 1.5mg/kg intravenous injection. Following stable hemodynamics in the postoperative period, the patient was extubated after 8 hours and discharged from ICU on the 5th postoperative day without any complications.
DISCUSSION
Percutaneous transluminal coronary angioplasty is very popular and is being used with increasing success to dilate proximal as well as distal coronary artery. Though the modern imaging technique has increased the success rate of the procedure; it is not always safe. Sometimes angioplasty equipment is fragmented and left behind in the coronary artery3,4 making the post-procedure period much more complicated. Usually this dislodgement or fragmentation may occur when a balloon catheter is inflated beyond its operating pressure range or undergoes mechanical stress like rotation, torsion during an attempt to dilate a resistant stenosis5. Fragmentation of balloon catheter or breakage of guidewire is rare. However, this complication can occur and fragmented part can remain in the coronary artery5 leading to severe hemodynamic instability. The incidence of dissection in interventional cardiology is less than 0.1% but in patient with LMCA disease it is much higher, nearly 1.05%6,7,8,9.
Drug eluting stents have revolutionized interventional cardiology these days, which may also dislodge from its mounted balloon or may have some problem during inflatation or deflation. In this case, it was a sirolimus-eluting stent of 2.5 x 29mm, which was left in LMCA due to mechanical failure of removal and coupled to it there was a problem of deflating it. A serious complication arises when entrapment or embolization of angioplasty balloons or guidewire occlude a coronary artery specially LMCA. It results the near total obstruction of coronary flow leading to acute coronary thrombosis with acute myocardial infarction and may lead to cardiac arrest if prompt removal is not done. So, it is a catastrophic complication and a real surgical emergency.
Balloon rupture is another catastrophic complication. It causes distal embolization of ruptured tip and also clot or calcific plaque dislodgement. In this case coronary artery may also rupture leading to hemorrhage as well as myocardial infarction. In the present case, multiple attempts of removal of balloon resulted in LMCA rupture, following that patient suffered from severe hypotension that was managed with fluid resuscitation and vasopressor infusion. Leakage of dye was seen in fluoroscopic angiography as unequivocal evidence. This led to emergency coronary artery bypass grafting (CABG) and subsequent removal of balloon. It was mentioned in many cases previously that emergency surgery for removal of broken or stuck parts of angioplasty instruments1,10,11,12 with emergency CABG was the last resort to save the patient.
As in this case, all such patients are receiving aspirin, clopidogrel, heparin and glycopeptide IIb-IIIa inhibitors, which increase the incidence of perioperative bleeding requiring multiple blood transfusions. As in emergency, vein graft is the choice of conduit in hemodynamically unstable patient; this patient received reverse saphenous vein grafts. In this patient retrograde cardioplegia was delivered as partially inflated balloon in the LMCA could have prevented the distribution of cardioplegia solution into the LAD and circumflex coronary artery13. It is really a nightmare to all interventional cardiologists as it is a life threatening complication if not promptly diagnosed and quickly treated with myocardial revascularization14,15,16,17.
Conclusion: Accidental rupture of left main coronary artery during percutaneous transluminal coronary angioplasty is a serious complication though rare. The essence of reporting this case is all interventional cardiologists must keep in mind that accidental rupture of left main coronary artery during angioplasty can cause sudden death if not intervened immediately and should be surgically managed when all noninvasive resorts yield no results.
Competing Interests: The authors have declared that no competing interests exist.
Authors’ Contribution: SKK – conception and writing; DD, CSD – supporting writers
REFERENCES
- Singh J, Thingnam SK, Das D, Singh H, Sharma R, Vijayvergia R. Surgical removal of entrapped and broken percutaneous transluminal coronary angioplasty balloon catheter. Interact Cardio Vasc Thorac Surg 2007;6:94–96.
[PubMed] [Free full text] doi: 10.1510/icvts.2006.140194 - Rosario PG, Donahoo JS. Coronary artery endarterectomy for retrieval of entrapped percutaneous angioplasty catheter. Ann Thorac Surg 1996;61:218–19[PubMed] doi:10.1016/0003-4975(95)00725-3
- Hartzler GO, Rutherford BD, McConahay DR. Retained percutaneous transluminal coronary angioplasty equipment components and their management. Am J Cardiol. 1987;60:1260–64.
[PubMed] doi:10.1016/0002-9149(87)90604-7 - Cheng LC, Lee J, Chic SW. A rare complication of PTCS: ruptured balloon with retained broken catheter. Ann Thorac Cardiovasc Surg. 2000;6:266–67. [PubMed]
- Colombo A, Skinner JM. Balloon entrapment in a coronary artery: potential serious complications of balloon rupture. Cathet Cardiovasc Diagn. 1990;19:23–25. [PubMed]doi: 10.1002/ccd.1810190107
- Kovac JD, de Bono DP. Cardiac catheter complications related to left main stem disease. Heart. 1996;76(1):76-8. [PubMed] [Free Full Text]
- Dunning DW, Kahn JK, Hawkins ET, O’Neil WW. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000;51(4):387-93 [PubMed] doi:10.1002/1522-726X(2000112)51:4
- Cheng CI, Wu CJ, Hsieh YK, Chen CJ, Chen SM, Yang CH, et al. Percutaneous coronary intervention for iatrogenic left main coronary artery dissection. Int J Cardiol. 2008;126(2):177-82. [PubMed] doi:10.1016/j.ijcard.2007.03.125
- Ertas G, Ural E, Van Der Giessen WJ. Successful stenting of catheter-induced unprotected left main coronary artery dissection. Cardiovasc J Afr. 2012;23(4):e6-7. [PubMed] doi: 10.5830/CVJA-2011-033
- Rosario PG, Donahoo JS. Coronary artery endarterectomy for retrieval of entrapped percutaneous angioplasty catheter. Ann Thorac Surg. 1996;61:218–19. [PubMed] doiI:10.1016/0003-4975(95)00725-3
- Matt P, Zerkowski HR, Pfisterer M, Brett W. Troubleshooting for a stuck Balloon-
Catheter. Ann Thorac Surg. 2007;83:320 [PubMed] [Free full text] - Yavuz S, Bozat T, Vural H, et al. Stent entrapment in ostium of left main coronary artery: emergency surgical removal. Asian Cardiovasc Thorac Ann. 1998;6:24041. [Free full text]
- Matt P, Zerkowski HR, Pfisterer M, Brett W. Troubleshooting for a stuck Balloon-Catheter. Ann Thorac Surg. 2007;83:320. [PubMed] [Free full text]
- Kovac JD, de Bono DP. Cardiac catheter complications related to left main stem disease. Heart. 1996;76(1):76-8. [PubMed] [Free full text]
- Dunning DW, Kahn JK, Hawkins ET, O’Neil WW. Iatrogenic coronary artery dissections extending into and involving the aortic root. Catheter Cardiovasc Interv. 2000;51(4):387-93. [PubMed]
- Cheng CI, Wu CJ, Hsieh YK, Chen CJ, Chen SM, Yang CH, et al. Percutaneous coronary intervention for iatrogenic left main coronary artery dissection. Int J Cardiol. 2008;126(2):177-82. [PubMed] doi: 10.1016/j.ijcard.2007.03.125
- Ertas G, Ural E, Van Der Giessen WJ. Successful stenting of catheter-induced unprotected left main coronary artery dissection. Cardiovasc J Afr. 2012;23(4):e6-7. [PubMed] [Free full text] doi: 10.5830/CVJA-2011-033
