
Saleem A Wani, Mamta Chadha, A Prakash, Shipra Aggarwal
Department of Anesthesiology, Northern Railway Central Hospital, Basant Lane, New Delhi-110055, India.
Correspondence: Dr Saleem A Wani, Department of Anesthesiology, Northern Railway Central Hospital, Basant Lane, Panchkuian Road, Near Connaught Place, New Delhi-110055, (India); E-mail: drsaleemwani@gmail.com; Phone: +919654480470
ABSTRACT
Objective: Carboprost is used to prevent postpartum hemorrhage in pregnant patients but is associated with severe nausea and vomiting .This a study was done to compare ondansetron and P6 point acupuncture stimulation for prevention of carboprost induced nausea and vomiting.
Methodology: Fifty ASA class I and II full term pregnant patients scheduled for elective cesarean section were randomly allocated into Group-O (n=25) and Group-P (n=25). Subarachnoid block (SAB) was administered in both groups using inj.0.5% hyperbaric bupivacaine in L3-L4 interspace to achieve a level between T4 to T6. Inj.carboprost 250 mcg was given intramuscularly after the delivery of anterior shoulder in both groups. In addition Group-O inj. Ondansetron was given and in Group-P acupuncture was applied at P6 acupoint. Mean arterial pressures were maintained within 20% of baseline. Both groups were observed for nausea and vomiting for two hours postoperatively.
Results: Overall incidence of nausea and vomiting was significantly less in Group-P than in Group-O, however, there was no significant difference in incidence of nausea and vomiting among the two groups when considered individually.
Conclusion: We conclude that stimulation of P6 point by acupuncture in comparison to ondansetron decreases the overall incidence of carboprost induced nausea and vomiting in the immediate postoperative period.
Key words: Carboprost, Cesarean section, Nausea and vomiting, P6 acupuncture, Ondansetron.
Citation: Wani SA, Chadha M, Prakash A, Aggarwal S. A comparison of ondansetron and P6 point acupuncture stimulation in prevention of carboprost induced nausea and vomiting in patients undergoing cesarean section under subarachnoid block. Anaesth Pain & Intensive Care 2015;19(1):24-17
INTRODUCTION
Nausea and vomiting is a frequent adverse effect seen with administration of carboprost tromethamine – a medication used to control postpartum hemorrhage. In spite of administration of potent antiemetics this side effect is difficult to control.
Acupuncture is a complementary medical therapy with its origin in China in which various diseases and disorders are treated with special fine needle punctures at strategic points called acupuncture points or acupoints for short, in the body. P6 is an acupuncture point in the body located 4 to 5 cm proximal to distal wrist crease between the tendons of flexor carpi radialis and palmaris longus. There are several studies which have shown a significant role of P6 acupoint stimulation in prevention of postoperative nausea and vomiting. However, most of these studies have assessed the efficacy of P6 stimulation in cancer chemotherapy induced nausea and vomiting. We were unable to locate a study comparing the efficacy of P6 acupuncture in prevention of emesis due to carboprost tromethamine in our literature search. Our objective in conducting this study was to compare intravenous ondansetron with P6 acupuncture stimulation in prevention of nausea and vomiting due to administration of carboprost in the immediate postoperative period.
METHODOLOGY
The study was approved by the hospital ethics committee and informed consent was taken from each patient. Exclusion criteria were emergency cesarean section, known allergy to any of the medications, abnormal liver and renal function tests, history of motion sickness or migraine, severe cardiac disease, history of maternal smoking, history of post-operative nausea and vomiting (PONV) in previous surgery and known asthma or epilepsy.
Fifty ASA I and II patients undergoing elective cesarean section were divided into Group-O (n=25) and Group-P (n=25). Both the groups were preloaded with 20 ml/kg of crystalloid solution. Standard American Society of Anesthesiology monitoring was done. Subarachnoid block was administered in both the groups with 0.5% hyperbaric bupivacaine using 25G Quincke’s needle. A T4 to T6 level of block was achieved in both the groups .Mean arterial pressures were maintained within 20% of baseline. In both the groups carboprost 250 µg was administered intramuscularly after the delivery of anterior shoulder of baby along with oxytocin 10 units in infusion. In Group-P acupuncture was done at P6 point immediately after giving subarachnoid block. Manual stimulation of acupuncture needle was done at 20 min intervals till the end of the procedure. In Group-O, inj. ondansetron 0.1 mg/kg was given IV slowly.
PONV was observed for two hours after end of surgery using the following grading:
Grade 0 = No nausea or vomiting
Grade 1 = only nausea.
Grade 2 = Nausea with retching.
Grade 3 = One episode of vomiting.
Grade 4 = More than one episode of vomiting.
Patients having more than one episode of vomiting were given a rescue therapy in the form of inj. dexamethasone 4 mg IV.
Neither the patient nor the person collecting data knew which group represented which type of treatment, making it a prospective randomized double blind study.
RESULTS
In the absence of any previous study, Cohen’s effect size was used to calculate sample size of two groups with a dichotomous outcome variable. To detect large scale effect size (0.8), the minimum required sample size with 80% power of study and two sided alpha of 5% was 25 patients per group. Total sample size taken was 50 with 25 in each group. Blocked randomization with sealed envelope method was used. In this technique, patients were randomized in a series of blocks of ten i.e. for every ten patients randomized, five received Group-O treatment and other five received Group-P treatment. The data was entered in MS excel spreadsheet and analysis was done using Statistical Package for Social Sciences (SPSS) version 21.0.The two groups were compatible with respect to demography, drug dosages and level of block (Table-I).Categorical variables were presented in number and percentage (%) and continuous variables as mean ± standard deviation (SD). Quantitative variables were compared using independent t-test between the two groups. Qualitative variable were compared using chi-square test / Fisher’s exact test. A p-value of <0.05 was considered statistically significant.
Table-I: Patient demographic characteristics and drug dosages:
|
Parameter |
Group – O (n=25) |
Group – P (n=25) |
p value |
|
Age (years) |
30.2 ± 3.83 |
29.28 ± 3.8 |
0.3981 |
|
Weight (kg) |
64.4 ± 5.7 |
64.64 ± 6.44 |
0.8896 |
|
Height (cm) |
155.19 ± 5.32 |
155.48 ± 5.23 |
0.8467 |
|
ASA Status(1,2) |
21,4 |
22,3 |
1 |
|
Bupivacaine dosage(mg) |
11.12 ± .94 |
12.02 ± .33 |
<0.0001 |
|
Level of block(T4/T6) |
19/6 |
17/8 |
0.7536 |
The incidence of nausea and vomiting was recorded in both groups for two hours following surgery (Fig 1).
Figure 1: Comparison of vomiting between the groups
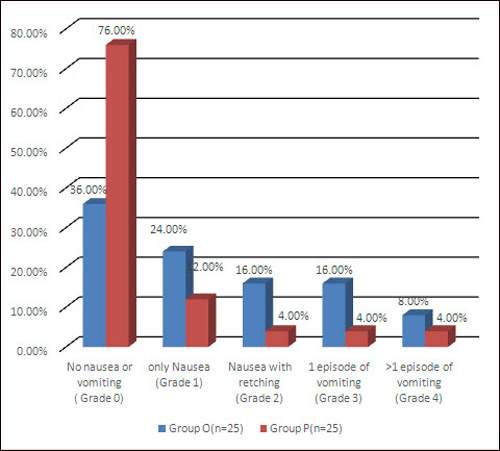
No nausea or vomiting was observed in nine patients in Group-O and in nineteen in Group-P, this was statistically significant (p-value=0.0096). Only nausea was observed in six patients in Group-O and in three patients in Group-P. Nausea with retching was seen in four patients in Group-O and in one patient in Group-P. Four patients in Group-O and one patient in Group-P had one episode of vomiting. More than one episode of vomiting occurred in two patients in Group-O and only one patient in Group-P. However, the incidence of patients having episodes of nausea or vomiting when considered individually was not statistically significant in two groups.
DISCUSSION
Carboprost tromethamine (PG-F2ᾳ analogue) is a synthetic prostaglandin used to control postpartum hemorrhage. One of the most distressing side effects after its administration is severe nausea and vomiting. Vomiting may cause dehydration, electrolyte imbalance, tension on suture lines, and increased risk of pulmonary aspiration especially if airway reflexes are depressed. Prophylactic medications used to control it have several adverse effects.
Non-pharmacological methods like acupuncture, acupressure and laser stimulation have shown comparable anti-emetic efficacy. These techniques have shown equal efficacy to commonly used anti-emetic drugs.1 Dundee et al in various studies found that acupuncture or acupressure at P6acupoint was as effective as a standard antiemetic in prevention of nausea and vomiting due to various causes.2-4
Cochrane systemic reviews in pooled data of trials including different antiemetics showed that P6 point acupuncture stimulation seemed to be superior to antiemetic medication for nausea and equivalent for vomiting. P6 stimulation was equally effective across different methods of stimulation, both invasive and noninvasive. The review showed superiority of P6 stimulation in chemotherapy induced nausea and vomiting in 11 trials and in more than 1200 patients.5
Acupressure at P6 was shown to cause a significant reduction in the incidence and severity of PONV twenty four hours after strabismus surgery which is similar to reduction seen with metoclopramide and ondansetron.6 An effectiveness study in 410 women showed that acupuncture stimulation may relieve nausea and vomiting after gynecological surgery.7 There is good clinical evidence from more than 40 randomized clinical trials that acupuncture has some effect in preventing or attenuating nausea and vomiting and a growing number of experimental studies suggest its mechanism of action.8-11 It has been observed that the incidence of PONV and requirement for rescue anti- emetics was significantly less in laparoscopic cholecystectomy patients in whom P6 acupressure was applied intraoperatively.12,13
In another study, Frey et al showed that P6 acustimulation can effectively decrease postoperative nausea and vomiting in high risk patients.14 Acupuncture or acupressure is as effective as an anti-emetic in prevention of cancer chemotherapy induced nausea and vomiting.2 Acupuncture combined with anti-emetics can effectively decrease the incidence and degree of cisplatin induced delayed nausea and vomiting.15
The mechanism of acupuncture is not clear. It is postulated that acupuncture causes stimulation of skin sensory receptors which may activate alpha, beta and delta fibres. These fibres synapse in the dorsal horn of spinal cord and in turn may cause release of endorphins from the hypothalamus. Increased levels of beta endorphins have been found in human CSF after acupuncture stimulation.16 In addition serotonergic and norepinephrenergic fibres may be activated. A possible change in serotonin levels has a role in prevention of nausea and vomiting17. Acupuncture has also been shown to enhance gastric motility .One recently done randomized controlled trial in critically ill patients showed that P6 acupuncture stimulation improved delayed gastric emptying18. Another suggested mechanism is the increase in vagal modulation which lessens the chances of nausea and vomiting10.
Acupressure (using sea bands) is free from side effects, economical and effective in reducing the severity of nausea and frequency of vomiting in pregnancy.18 Zheng H et al in their study found that transcutaneous electric stimulation of P6 acupoint could prevent nausea and vomiting induced by patient controlled intravenous analgesia with tramadol.19 Acupressure at P6 has also been shown to reduce the radiation therapy related nausea significantly.20
For acupuncture to be effective, it has to be applied prior to emetic stimulus and correct point location.21 Acupuncture is increasingly used in west for chronic pain, musculoskeletal disorders, headache, migraine and other disorders in which modern western medicine is less effective. Alternative and complementary procedures are considered promising areas of research and application about which much remains to be learned.
Our study demonstrates that acupuncture at P6 acupoint in comparison to ondansetron significantly decreases the incidence of nausea and vomiting when considered together as a carboprost induced complication. But no significant difference was seen between P6 acupuncture and ondansetron in preventing nausea and vomiting when considered individually as a complication. However, we strongly believe that if the sample size was increased, the differences between the two groups may become significant when nausea and vomiting are considered as individual complications.
CONCLUSION
Acupuncture stimulation at P6 was found to be more effective than ondansetron in prevention of carboprost induced nausea and vomiting in patients undergoing cesarean sections done under subarachnoid block.
REFERENCES
- Lee A, Done ML. The use of non pharmacological techniques to prevent postoperative nausea and vomiting: A meta analysis. Anesth Analg 99;88:1362-9. [PubMed]
- Dundee JW, Ghaly RG, Fitzpatrick KT, Lynch G, Abram P. Optimizing anti-emetics in cancer chemotherapy. BMJ 1987;294:179.[PubMed] [ Free full text]
- Dundee JW, Ghaly RG, Bill KM, Chestnutt WN, Fitzpatrick KT, Lynas AG. Effect of P6 stimulation on postoperative nausea and vomiting. Br J Anaesth 1989;63;612-8 . [PubMed]
- Dundee JW, Sourial FB, Ghaly RG, Bell PF. P6 acupressure reduces morning sickness. JR Soc Med 1988;81:456-7. [PubMed][Free full text]
- Ezzo J, Streitberger K, Schneider A. Cochrane systemic reviews examine P6 acupuncture stimulation for nausea and vomiting. J Altern Complement Med 2006;12:489-95. [PubMed]
- Soltani AE, Mohammadinasab H, Goudarzi M, Arbabi S, Mohtaram R, Afkham K, et al. Acupressure using ondansetron versus metoclopramide on reduction of post operative nausea and vomiting after strabismus surgery. Arch Iran Med 2010;13:288-93. [PubMed][Free full text]
- Alkaissi A, Evertsson K, Johnson VA, Ofenbart L, Kalman S. P6 Acupressure may relieve nausea and vomiting after gynaecological surgery : an effectiveness study in 410 women. Can J Anaesth 2002; 49:1034-9. [PubMed]
- Streitberger K, Ezzo J, Schneider A. Acupuncture for nausea and vomiting – an update of clinical and experimental studies. Auton Neurosci 2006;129;107-17 . [PubMed]
- Han JS. Acupuncture and endorphins. Neurosci lett 2004;361:258-61. [PubMed]
- Huang ST, Chen GY, Lo HM, Lin JG, Lee YS, Kuo CD. Increase in vagal modulation by acupuncture and neiguan point in the healthy subjects. Am J of Chin Med 2005;33:157-64. [PubMed]
- Pfab F, Winhard M, Nowak-Machen M, Napadow V, Irnich D, Pawlik M, et al. Acupuncture in critically ill patients improves delayed gastric emptying- randomised control trial. Anesth Analg 2011;112:150-5. [PubMed][Free full text]
- Agarwal A, Bose N, Gaur A, Singh U, Gupta MK, Singh D, et al. Acupressure and ondansetron for postoperative nausea and vomiting after laparoscopic cholecystectomy. Can J Anaesth 2002;49:554-60. [PubMed]
13. Frey UH, Funk M, Lohlein C, Peters J. Effect of P6 acustimulation on PONV in patients undergoing laparoscopic cholecystectomy . Acta Anaesthesiol Scand 2009;53:1341-7. [PubMed]14. Frey UH, Scharmann P, Lohlein C, Peters J. P6 acustimulation effectively decreases nausea and vomiting in high risk patients. Br J Anaesth 2009;102:620-5. [PubMed]15. Sima L, Wang X. Therapeutic effect of acupuncture on cisplatin induced nausea and vomiting. Chinese acupuncture and moxibustion 2009;29:3-6. [PubMed]16. Ciement-Jones V, McLaughlin L, Tomlin S, Besser GM, Rees LH, Wen HL. Increased beta endorphin levels but not metenkephalin levels in human cerebrospinal fluid after acupuncture for recurrent pain. Lancet 1980;1:946-9. [PubMed]17. Pomeranz B. Scientific basics of acupuncture. In: Stux G, Pomeranz B, eds. Acupuncture Textbook and Atlas. Heidelberg: Springer-Verlag;1987: 1-18.
18. Khavandizadeh AS, Mehfouzi B. Evaluation of the effects of acupressure by sea band on nausea and vomiting of pregnancy. Iranian Journal of Obstetrics, Gynaecology and Infertility 2010;13:39-44. [Online]
19. Zheng LH, Sun H, Wang GN, Liang J, Wu HX. Effect of transcutaneous electrical acupoints stimulation on nausea and vomiting induced by patient control intravenous analgesia with tramadol. Chin J Integr Med 2008;14:61-4. [PubMed]20. Roscoe JA, Bushunow P, Jean Pierre P, Heckler CE, Purnell JQ, Peppone LJ, et al. Acupressure bands are effective in reducing radiation therapy related nausea. J Pain Symptom Manage 2009;38:381-9. [PubMed][Free full text]21. Dundee JW, Ghaly RG. Does the timing of P6 acupuncture influence its efficacy as a post- operative anti-emetic? Br J Anaesth 1989;63:630.
